Acute polymorphic psychotic disorder belongs to the category of transient (transient) psychotic disorders. Its main feature is its sharp, characteristic bright beginning. Within a period of up to two weeks, a person abruptly goes from a non-psychotic state to a psychotic one. The patient experiences productive symptoms - hallucinations and delusions.
Non-psychotic polymorphic disorder can become psychotic at any time
Story
The existence of acute short-term psychoses with an extremely severe course and complete remission was recognized and well described by almost all major psychiatrists of the pre-Kraepelin era [1]. After E. Kraepelin identified the group of endogenous psychoses in 1899 and its dichotomy dementia praecox - manic-depressive psychosis, various acute psychoses fell into both of these categories. However, Emil Kraepelin himself argued that there is a “considerable group of disorders” [1] that cannot be classified according to this principle.
With the advent of E. Bleuler’s concept of “schizophrenia” in 1908 and the improvement of Kraepelin’s classification, the problem of acute, short and transient (transient) psychoses with a favorable prognosis was still not resolved [1].
Concepts opposed to Kraepelin and Bleuler led to the identification of a special group of psychoses, different from schizophrenia and bipolar disorder and, in part, schizoaffective disorder, which in the respective countries had the name traditional for the national school of psychiatry [1]:
- Cycloid psychoses
: Germany; - fr. Bouffée délirante
(delusional outbreak): France; - Reactive or psychogenic psychoses
: Scandinavian countries (Denmark, Finland, Iceland, Norway, Sweden); - Atypical psychoses
: Japan; - Certain forms of reactive psychoses (for example, reactive paranoid
,
paranoid reaction
): USSR[2][3].
Other historical names for acute and transient psychotic disorders:
- Acute (undifferentiated) schizophrenia, acute schizophrenic episode;
- Oneirophrenia;
- Psychogenic (paranoid) psychosis;
- Schizophrenic reaction;
- Schizophrenia with a favorable prognosis.
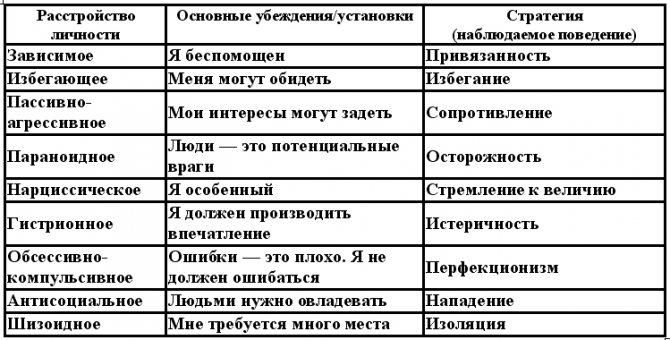
Types of Personality Disorders
Personality disorder refers to mental disorders. Usually this is a whole complex of behavioral signs, characterized by striking deviations from generally accepted norms due to the patient’s distorted perception of objective reality. There are no “bad” personality types, there are successful and unsuccessful conditions for their existence, which give a harmonious, happy life or, conversely, a depressing and gloomy life. Most personality disorders require psychotherapeutic treatment. Some of them begin in early childhood and even at birth.
So, the following types of personality disorders are distinguished:
- dependent (search for and binding to a guardian who will bear full responsibility for the actions taken);
- avoidant (people are afraid of being rejected and abandoned after a short relationship, so they live alone so as not to be disappointed);
- passive-aggressive (people who crave freedom of action, but cannot cope with it);
- paranoid (distrust of other people, high demands on them, but not on oneself);
- obsessive-compulsive (people who are used to controlling and criticizing everything);
- antisocial (sociopaths);
- narcissistic (narcissism);
- schizoid (living in isolation);
- histrionic (they like to make contact with others, are intrusive and overly vigilant).
It is clear that all personality disorders affect social adaptation in one way or another. Along with this, functional disorders occur in the main areas:
- emotions;
- perception;
- thinking;
- behavior;
- interpersonal relationships.
Often there is a substitution of concepts, which distorts the overall picture of the perception of the world as a whole, a person’s principles and approaches change, but the revaluation of values and improvements caused by the useful information load, which is necessary in such cases, does not occur.
Accordingly, behavior has also changed, which usually so noticeably affects the existence and definition of oneself in society. The patient’s lifestyle changes beyond recognition, oppressing him, but sometimes without the help of loved ones the patient cannot cope with the illness and resume normal life activities.
Classification
General diagnostic guidelines for acute and transient psychotic disorders in the International Classification of Diseases, 10th Revision (ICD-10)[4]:
- acute onset (up to two weeks), with the development of hallucinations, delusions, incoherent or broken speech, which appear alone or in any combination;
- if confusion, false recognition or disturbances of attention are present, they do not meet the criteria for organically caused clouding of consciousness;
- not consistent with a depressive episode, manic episode, or recurrent depressive disorder;
- psychotic disorder is not associated with substance use;
- Organic brain disease and serious metabolic disorders affecting the central nervous system (except childbirth) are excluded.
The fifth character in the classification indicates the association of the acute onset of a psychotic disorder with acute stress occurring within 2 weeks before the development of acute psychotic symptoms (i.e., F23.x0 - without combination with acute stress, F23.x1 - in combination with acute stress).
The following subcategories are distinguished:
- 23.023.0 Acute polymorphic psychotic disorder without symptoms of schizophrenia.
- 23.123.1 Acute polymorphic psychotic disorder with symptoms of schizophrenia.
- 23.223.2 Acute schizophrenia-like psychotic disorder
- 23.323.3 Other acute predominantly delusional psychotic disorders.
- 23.823.8 Other acute and transient psychotic disorders.
- 23.923.9 Acute and transient psychotic disorder, unspecified.
What are acute psychotic disorders?
There are two main types. This:
- acute polymorphic psychotic disorder without symptoms of schizophrenia;
- acute polymorphic psychotic disorder with symptoms of schizophrenia.
No symptoms of schizophrenia
If without (F23.0x), then despite all the variety of types of hallucinations and delusions, the rate of their change, the patient should not have symptoms of schizophrenia. In the case of a protracted course of the disorder, the diagnosis changes. Most likely chronic delusional disorder or another non-organic delusional disorder. But not for schizophrenia.
How does psychotic disorder F23.0 manifest? In addition to the abrupt onset, patients must have hallucinations and delusions of several types. They change throughout the day and even literally before our eyes. There should also be sudden mood swings.
Schizophrenia of all forms is excluded. There is no rich symptom complex. Both phases of bipolar affective disorder are also excluded. In reference books you can read that the symptoms present must differ from those present in schizophrenia. This is not entirely true from a practical point of view. Distinguishing between carnivorous cats of gigantic stature in all types of delusional disorders is not a very rewarding task. It’s better to say this... These cats do not exist in people diagnosed with “Paranoia”. Those have great discoveries and are jealous of their wives or husbands. Cats in people with paranoid schizophrenia, with a psychotic disorder of a transient type without symptoms of schizophrenia and with them can be similar, as well as the behavior of those who see such outrages. Something definite can be established from the very history of life and disorder. Transient ones are most often caused by stress - big, bright and understandable. Well, then - time will tell. For transient disorders, you can do without antipsychotics. Sometimes everything goes well at the level of first line of therapy -
- general and supportive;
- sedatives;
- means that normalize sleep.
Most often there are fantastic delusions and delusions of staging, but there may be some elements of delusions of persecution and damage. Only usually they acquire fantastic features.

Delusions in polymorphic psychotic disorder acquire fantastic features
With symptoms of schizophrenia
Acute polymorphic psychotic disorder with symptoms of schizophrenia (F23.1x) does not differ in appearance from paranoid schizophrenia. If you observe two patients diagnosed with F20.0 and F23.1, they can be almost completely identical. Moreover, a disorder of this type may include Kandinsky-Clerambault syndrome, which would make the situation completely the same.
The difference is the abrupt onset, which is associated with a major traumatic event. Theoretically, this could even be some kind of idea. In practice, such an event is the death of a loved one, sudden bankruptcy, or the commission of some terrible action towards the patient or the patients themselves. So, one of the patients hit pedestrians, killing a child. Out of deep emotion, he disappeared from the scene of the event, tried to commit suicide, but hallucinations began, and a harmonious outline of false fantastic causes and consequences arose. This is already a symptom of schizophrenia. Otherwise, with F23.0, he could see bloody boys in his eyes, but look for some fantastic pests in the garage, and hide and disguise himself along the way, line up the plot, give it reasonable features... Yes, and hid- when he ran to the garage, what? Head. He was sure that his thoughts could be heard by everyone, and the police would use them to identify him. Therefore, you need to find evidence of pest activity in the garage as soon as possible. And at the same time, he considered himself guilty, but that he did not look closely, did not check the car. These are already symptoms of paranoid schizophrenia, but not itself. Subsequently, he admitted his guilt, but in the hit-and-run, and the lawyer managed to prove that he left the place due to a sudden mental disorder. Not just stress, but a complex condition.
Worth Seeing: Generalized Anxiety Disorder
If improvement does not occur within a month, then the diagnosis is changed to schizophrenia and noted with code F20.xxx.
So, this is a sharply emerging delusion with features of delirium in schizophrenia spectrum disorders, hallucinations, mental automatisms, cycloid psychosis with symptoms of schizophrenia. All criteria may not be observed at once.
Why was the patient who ran over pedestrians diagnosed with “polymorphic psychotic disorder” and not schizophreniform? The fact is that there was only a short-term outbreak. In the evening he came to his senses. Relatives and a lawyer recommended contacting psychiatrists. At night the hallucinations returned. He didn't understand what he was seeing. A dream, or he sees how “pests” are damaging his car, filing something in the steering, which is why he jerks the steering wheel. In the morning he came with friends to the hospital and told about what had happened. The man did not think of escaping responsibility, but the help of psychiatrists was actually needed. But this is just a flash. They don’t say about this that it’s a premiere or an episode. Is the episode lasting less than a day? This is too low even for schizophreniform disorder. During the day, during the admission and hospitalization, signs of delirium still persisted and there was a derealization effect, but there were no longer hallucinations. There was something similar to a delusional idea, but the life situation itself, of course, contributed to this without any miracles of mental disorders. The “jumps” in mood also persisted for a very long time. I was afraid of hallucinations and that they would come back. But this is quite understandable...

Acute polymorphic psychotic disorder may be accompanied by symptoms of schizophrenia
Schizophreniform acute disorder
The same group of transient acute disorders includes schizophreniform. We are already beginning to understand the difference from what constitutes an acute psychotic disorder of a polymorphic type with symptoms of schizophrenia. The episode will last about a month, the symptoms are more stable and in themselves do not differ in any way from the symptoms of the paranoid form.
To what constitutes a polymorphic psychotic disorder with symptoms of schizophrenia, one can safely add the oneiric state, a deeper plot of delirium. Signs of catatonia may also be observed - stupor or stereotypical movements. From schizophrenia itself, you need to take away the prodrome period and change the duration of the course, shorten it to a month, and then you get schizophreniform disorder.
Epidemiology
According to the HASBAP study, acute and transient psychotic disorders account for 4% of the total group of non-organic psychoses and affective disorders (in ICD-10 - categories 2. and 3.) [1]. If affective disorders are excluded, their share will be 8.5%[1].
This group of diseases is significantly more often diagnosed in women (female:male ratio = 78.6%:21.4%)[1]. This significantly distinguishes acute and transient psychotic disorders from schizophrenia, for which the risk of development does not differ between men and women[6].
This diagnosis is the most common during the patient’s initial hospitalization in the emergency department[5]:167.
Against the backdrop of alcoholism...
Alcohol brings some difficulty in diagnosing and developing treatment methods. Mental and behavioral disorders due to alcohol use are intoxication itself, alcoholism itself and the delirium it causes. It may be completely no different or almost no different from acute and transient mental disorders. Alcohol and mental disorders are linked so tightly that they cannot be broken. Delirium tremens most often begins when a person suddenly stops drinking, which means that he will end up in the hospital sober. The main criterion for differentiating delirium delirium and transient disorder F23 is, again, alcoholism itself. There are just no clear rules here. In psychiatry, hospitalization occurs based on the presence of psychosis. But no one will say that the delirium of an alcoholic is not psychosis. Therefore, patients may end up in drug addiction treatment or in a psychiatric hospital. All that is taken into account is that the alcoholic also needs drug treatment. What will be recorded in the medical history if the patient has been drinking and now has hallucinations? Something from block F10-F19, depends on the situation.
But this does not mean that the disorder is caused precisely by alcoholism, although it, of course, simply cannot help but create some kind of complicating or provoking background. Someone is diagnosed with F23.0. Don't assume they are all teetotalers. It’s just that other factors come first for them; the main problem is not alcoholism and refusal from it.
Worth seeing: Dissociative anesthesia