Atypical facial pain
Pain that does not fit into the description of neurogenic, autonomic, musculoskeletal prosopalgia is classified as atypical facial pain . As a rule, their atypicality is associated with the simultaneous presence of signs characteristic of several types of pain syndromes, but the psychopathological component usually dominates.
SYMPTOMS AND DIAGNOSIS
One type of atypical facial pain is persistent idiopathic facial pain. The pain can be triggered by surgery on the face, trauma to the face, teeth or gums, but its persistence cannot be explained by any local cause. The pain does not meet the diagnostic criteria for any of the described forms of cranial neuralgia and is not associated with any other pathology. Initially, pain occurs in a limited area on one side of the face, for example, in the nasal fold or one side of the chin. In some cases, patients cannot accurately localize their sensations at all. In the area of pain, no sensitivity disorders or other organic disorders are detected. Additional research methods do not detect any clinically significant pathology. Another form of atypical facial pain is atypical odontalgia. This term is used to refer to prolonged pain in the teeth or bed after tooth extraction in the absence of any objective pathology. This syndrome is close to the so-called “dental plexalgia”. Among the patients, women of menopausal age predominate (9:1). Constant burning pain in the area of the teeth and gums is typical, often with repercussion to the opposite side. There are usually no objective signs of dental or neurological disorders, although in some patients the syndrome develops after dental procedures (simultaneous removal of several teeth or filling material extending beyond the apex of the tooth). In some cases, a decrease in pain during eating is observed and an increase in pain under the influence of emotions, adverse meteorological factors and hypothermia. When the superior dental plexus is damaged, pain can radiate along the second branch of the trigeminal nerve and be accompanied by autonomic symptoms, likely resulting from connections between the plexus and the autonomic ganglia (pterygopalatine ganglion and superior cervical sympathetic ganglion). As a rule, there is no pain at the exit points of the branches of the trigeminal nerve and no pronounced sensory disturbances in the zones of innervation of its II and III branches. Bilateral dental plexalgia develops almost exclusively in women after 40 years of age and has a long course. Burning pain usually appears on one side, but soon appears on the opposite side. Almost all patients develop pain on both sides within 1 year. The simultaneous development of bilateral pain is also possible. As with unilateral dental plexalgia, the upper dental plexus is affected 2 times more often than the lower one.
CAUSES
Possible etiological factors of bilateral dental plexalgia include complex removal of wisdom teeth, premolars and molars, conduction anesthesia, osteomyelitis of the sockets, surgical interventions on the jaws, entry of filling material into the mandibular canal through the root canals of the teeth, removal of a large number of teeth in a short period of time during preparation of the oral cavity for prosthetics, infection, intoxication, mental trauma, etc.
TREATMENT
Treatment should be carried out exclusively by a neurologist. Self-medication is unacceptable.
How does the attack go?
A classic attack of neuralgia usually goes like this: a severe shooting pain appears, which the patient compares to an electric shock; the duration of pain is two minutes; the duration of the interval between attacks directly depends on the stage of the disease that caused it; the area of localization of pain will not change for several years; the pain always has the same direction (it appears in one area and goes to another); there are areas on the patient’s face, when irritated, characteristic pain appears; the presence of certain factors that influence the occurrence of pain; the patient’s special behavior during an attack (he does not cry or move, but, on the contrary, freezes in the position in which the pain overtook him - some begin to immediately rub the affected area); At the peak of pain, the facial muscles may begin to twitch.
Migraine
Migraine attacks occur in approximately fifty percent of the world's inhabitants. Their true cause has not yet been established. Migraines are characterized by unilateral pain. Patients usually complain that the left side of their face or, conversely, the right side hurts.
- dizziness;
- weakness;
- the side of the face and eyes hurt;
- increased sweating;
- nauseating feeling;
- absent-mindedness;
- sensitivity to bright lights and loud sounds.
Paroxysmal cluster pains appear unexpectedly. Most medical professionals associate them with psychological problems. Most often, painful manifestations occur in men. At the same time, the intensity of the pain is very strong - the patient feels lumbago and pulsation in the temples and facial area. The duration of attacks ranges from half an hour to three days.
The face and head often hurt when you have a cold. In this case, the patient additionally notes:
- red face;
- increase in body temperature to thirty-eight degrees;
- muscle weakness;
- Half of the face and eyes hurt;
- increased sweating;
- lack of appetite.
Elevated blood pressure results in impaired blood supply to the cerebral cortex. In this case, the cells of the central nervous system experience oxygen starvation, as well as nutritional deficiency. In such conditions, the head, including the face, suffers greatly. Stabilizing the indicator will eliminate unpleasant sensations.
Soreness often occurs with ophthalmic disorders. A condition where the face hurts and the head can appear with:
- working at a computer for long periods of time or watching television for many hours;
- glaucoma;
- pterygium;
- blepharitis;
- conjunctivitis.
In such cases, it is necessary to consult an ophthalmologist.
Whatever the reasons for the condition when your face hurts, you cannot ignore it. Only under the supervision of an experienced specialist can pathological symptoms be eliminated and health maintained.
The skin of the face may hurt in the following cases:
- There was a soft tissue injury.
- A malignant tumor develops on the face - melanoma. Often this neoplasm appears from a mole when its cells degenerate.
- Acne, that is, blackheads, can hurt. This is especially true for rashes that are located deep under the skin. You can get rid of acne using antiseptic and antibacterial creams and lotions. You need to take proper care of your skin.
- An allergic reaction such as angioedema may be accompanied by facial pain. At the same time, the person’s eyes and soft tissues become red and watery. The larynx becomes very swollen, which can lead to suffocation.
Sometimes facial pain can be associated with reasons that are not related to any diseases. Thus, the face and scalp may hurt due to wearing elastic bands and hairpins that are too tight.
The jaw hurts and clicks after prosthetics or dental treatment
Dysfunction of the temporomandibular joint. The lower jaw is connected to the skull by two temporomandibular joints. Impairment of the function of these joints is possible after the installation of a denture, crown, bridge, any treatment or tooth extraction if this leads to malocclusion and/or damage to the temporomandibular joint. This is a typical complication after dental prosthetics. Read more about treating TMJ dysfunction here
Temporomandibular joint dysfunction
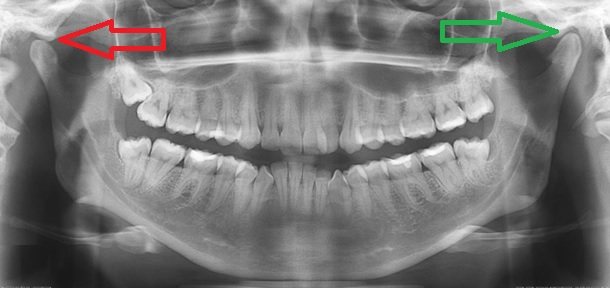
The green arrow indicates a healthy joint. The red arrow points to the joint that remains in the “open” position when the mouth is closed. This leads to wear and tear of the articular cartilage, pain and clicking when opening and closing the mouth. One of the reasons is the incorrect position of the upper right “eight” (tooth 1_8 lies horizontally).
How can we help you:
- Anti-inflammatory treatment will help relieve pain. If necessary, we inject anti-inflammatory medication directly into the lower jaw joint . This brings relief within a few minutes .
- Injection of botulinum toxin preparations (for example, Botox or Dysport) into spasmodic muscles. This is relevant in the case of an excessive increase in the tone of the masticatory muscles, if it is the muscles that are the “culprit” of dysfunction of the temporomandibular joint.
- Treatment by an osteopath. An osteopath works with the joints and muscles of the jaw using gentle manual techniques. This way you can solve a lot of problems that cannot be solved in classical dentistry. More about osteopathy
- Introduction of chondroprotectors (medicines for nutrition and restoration of cartilage) into the temporomandibular joint. Read more about cartilage restoration
How to get rid
muscle relaxants, analgesics, nootropics.
Neck massage, physiotherapy, and acupuncture are required. Treatment is prescribed only when the diagnosis is confirmed. Self-diagnosis in this case is unacceptable.
The drugs of choice are most often carbamazepine and amitriptyline. The first is to take 0.1 grams twice a day. Gradually the daily dose has to be increased. After 6 - 8 weeks from the onset of a positive effect, the dose should be reduced and made maintenance, that is, back to what it was at the very beginning.
The second drug, which is an antidepressant, is prescribed at a dose of 200 mg per day and only with meals. After a lasting effect occurs after a month, the dosage should be reduced.
Milgamma is a complex vitamin preparation that has a pronounced positive effect on the nervous system. The course should be taken several times a year.
Where is atypical facial pain treated? Most often, the patient needs inpatient treatment, so therapy is mainly carried out in a neurological department. Sometimes the intervention of a psychologist may be required. In this case, therapy is also carried out in a specialized hospital.
Treatment
It is necessary to treat emerging facial pain depending on the causes of its occurrence.
- during the development of symptomatic pathology, otitis media, sinusitis, and pulpitis should be treated;
- neurogenic, vascular and myogenic are treated with anti-inflammatory drugs, but only if the pain occurs due to the inflammatory process, physiotherapeutic therapy is also used: ultraphonophoresis, magnetic therapy, electrophoresis;
- to block pain at the points where it manifests itself, it is necessary to carry out therapeutic blockades - for this, local anesthesia is administered;
- It is better to block trigeminal neuralgia with ganglion blockers;
- Horton's disease is treated with corticosteroids;
- compressive prosopalgia, that is, facial, is treated not only with medications that relieve inflammation, but also with vascular therapy, drugs that relieve swelling, and B vitamins are prescribed.
If the use of medications does not produce the expected result, then the patient is prescribed surgical treatment. In particular, this is microsurgery for decompression of the trigeminal nerve. In case of persistent pathology during the development of ganglioneuritis, the affected nerve node is removed.
The trigeminal form is treated with radiofrequency destruction of the endings of the trigeminal nerve.
For each form of prosopalgia, sedatives are required. For this purpose, antidepressants, sedative herbal preparations, and mild tranquilizers are used.
If necessary, vegetotropic medications are prescribed.
The psychogenic type is eliminated with the help of psychotherapy, individually selected psychotropic drugs. This includes tranquilizers, antidepressants and others. The patient is prescribed electrosleep and darsonvalization. To determine its deviations, a “depression scale” is used.