Behavioral symptoms of dementia
Manifestations of dementia vary from person to person. They depend on the nature of the brain disorder, temperament, and personality traits of the patient. Progressive dementia reduces the cognitive (mental) function of the brain, negatively affects the psycho-emotional sphere, and leads to changes in behavior.
All changes occur in parallel. Deviations in behavior accompany changes in the psyche and memory. They are found at all stages of the disease. For each stage, a number of typical sets (clusters) of behavioral manifestations can be identified.
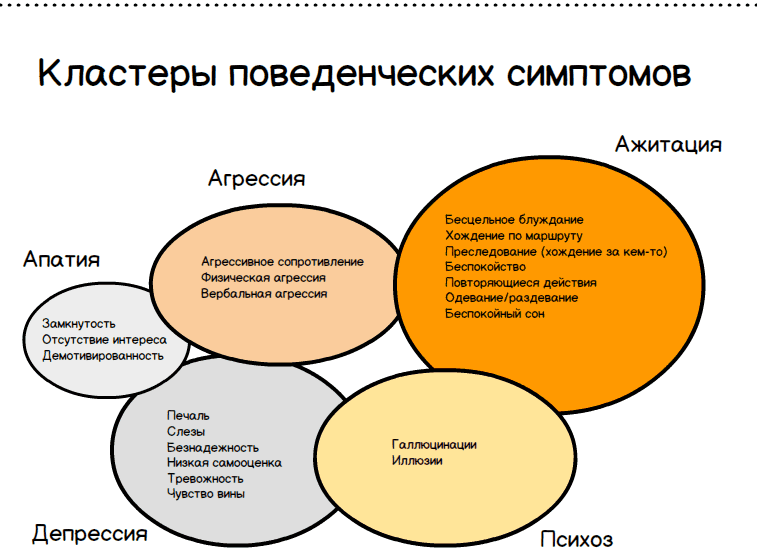
The sets of symptoms, regardless of the cause of the brain disorder, are almost universal. There are 5 main clusters:
- Apathy. Lack of interests, desires.
- Agitation. Aimless wandering, fussiness, repetitive movements.
- Aggression. Physical, verbal, stubborn resistance.
- Depression. Tearfulness, sadness, hopelessness, low self-esteem, anxiety, guilt.
- Psychosis. Auditory, visual hallucinations, mania.
At all stages of the disease, apathy may spontaneously occur. This cluster is most common in dementia and is observed in all types. Common manifestations of the disorder include depression, which can be triggered, in particular, by placement in a nursing home or inadequate nursing care at home.
Depression and apathy are observed in mild stages of dementia and cognitive impairment. Aggression, agitation and psychosis usually occur at the stage of moderate and severe forms of the disease.
Agitation is more often observed with frontotemporal degeneration, depression is more often provoked by the vascular form of dementia, psychosis occurs more often with dementia with Lewy bodies.
Why is proper nutrition important for dementia?
In most cases, dementia is caused by organic changes in brain tissue. The nutrition of neurons deteriorates, connections between them are disrupted, and individual areas die off. There may be several reasons leading to this, but most often the primary source is poor blood supply due to problems with blood vessels.
Substances supplied with food simply do not reach the brain tissue due to impaired metabolism. The nervous system, which does not receive a large amount of vitamins, slows down its work. The already existing symptoms of the disease worsen, and new ones join them. The underlying disease develops rapidly.
But the nutrition of patients with dementia affects not only their mental but also their physical state. Due to improper food intake (too frequent or, on the contrary, rare), the functioning of the gastrointestinal tract is disrupted. Difficulty swallowing prevents you from eating foods in their usual form. Problems with bowel movements and vomiting in dementia are quite common accompanying symptoms.
Characteristics of behavioral symptoms
Typical behavioral manifestations include agitation (motor restlessness). This behavior disorder occurs in 50% of patients with acquired dementia, and the manifestation acquires clinical significance in 20% of patients.
At the early stage of the disease, agitation is manifested by senseless shifting of objects, walking back and forth, growing internal tension, which breaks through with sighs, screams, and groans.
After 65 years, apathy, a state of suppressed emotions, and depression, a mental disorder associated with the loss of the ability to enjoy, are considered an early sign of a developing disease. Depression is found in 20% of people with dementia, and the majority show some signs of depression. You can determine your level of depression using the Beck test.
Manifestations of depression in dementia.
Rare: melancholy, suicidal ideation, diurnal mood swings
More often: aggressiveness, uncontrollable crying, agitation, irritability, negativity, refusal to eat
Verbal and physical aggression is observed, according to various estimates, in 33-46% of people suffering from dementia. Aggression arises due to the inability to explain one’s needs in the usual way. Reproaches, threats, pinching, hitting and other similar manifestations mean that a person is experiencing pain, cold, heat, hunger or another uncomfortable state.
Acute and chronic psychosis develops with severe brain disorder as a result of massive death of nerve cells. The condition is characterized by jealousy, delusions, suicidal tendencies or causing damage to things or other people.
Up to 20% of patients with dementia suffer from psychosis. The most common delusional ideas in dementia include theft, jealousy, poisoning, and being left without help.
Alzheimer's disease and aggressive behavior: what to do? Agitation in people with dementia
Caring for a patient with dementia as if he does not understand or feel anything is a big mistake, but it is one that staff in nursing homes for the elderly often make.
Aggressive behavior sometimes accompanies Alzheimer's disease simply because the person with dementia is treated like a thing.
How can caregivers of patients with memory loss respond to aggressive outbursts?
Shortly after Margie was diagnosed with early-stage Alzheimer's disease at age 57, she began experiencing frequent attacks of anxiety and paranoia, running away from home and getting lost several times. Her husband Pete and daughter Jennifer even had to turn to the police for help.
After one of these incidents, Pete himself was taken to the hospital with high blood pressure. The constant stress common when caring for someone with memory loss took a toll on his physical health. In the end, he had to accept the painful thought that Margie needed more help.
Margie was placed in a boarding house for people with memory impairment, but the process of adapting to the new place was difficult. Local staff did not know how to manage the type of behavior that Margie's dementia caused - anxiety, anger, aggression. The situation was getting worse. After Margie pushed and punched a nurse who was trying to help her shower, Pete turned to me for help.
Unfortunately, this situation is quite typical for institutions that do not pay due attention to training employees in methods of communication with patients.
As a result, staff are unable to gently and caringly manage the behavior of the person with dementia. I agreed to spend a few hours with Margie.
My plan was to observe her and then talk to the staff and offer them options on how to deal with her agitation and aggression.
Back to contents
Aggressive behavior in Alzheimer's disease: there are reasons for everything
When I arrived, Margie was in the common room with a group of other patients playing something. She sat at the table with everyone, but did not participate in the general activities at all. After a few minutes, Margie stood up. She spent most of her waking hours wandering up and down the corridors. Margie slept very little and hardly sat still for a minute.
Margie's daughter Jennifer introduced me to her as someone she knew. Pete came with us too and kissed Margie. She smiled at them both and said hello to me.
While talking, we walked along the corridors and sat down in the lobby for a few minutes. It was clear that Margie was uncomfortable sitting for long periods of time.
Pete explained that she had a bad back, and I suggested that this might be one of the reasons for her constant movement.
After forty-five minutes of walking the halls with Margie, I noticed that it was time for the staff to change her: she was incontinent. Walking past the nurse's station, I quietly reported this so that Margie wouldn't hear. The nurse asked us to take Margie to her room and promised to send someone to help her.
The room was narrow and long, with three beds, which were separated from each other by curtains; Margie's bed was the furthest from the entrance. When we entered, Margie's calm and even mood gave way to suspicion - like that of a frightened victim. She became alarmed and gave me an unexpectedly incredulous look.
I turned to go out into the hallway as two nurses came into the room to change Margie. They walked resolutely to her bed and drew the curtain. Less than two minutes had passed when Margie rushed out into the corridor with her trousers unbuttoned and her face red with indignation. She screamed, swore and threatened that she would never enter the ward again.
Margie ran to the nurses' station, grabbed a stack of books, and threw them at the nurse. Pete and I walked up behind her and, as gently as we could, began talking to her and stroking her arms. This method always helped Pete out when he needed to calm down an agitated Margie. Jennifer was then able to take her into the hall and finally calm her down.
I asked my sister if it would be possible to have a woman change Margie's clothes - it was obvious that she was afraid of the nurses. The nurse replied that this was impossible due to scheduling difficulties - there were not enough nurses for each shift.
In addition, as she explained to us, changing Margie had to be done by men strong enough to “hold her in the process.” This answer shocked Pete, Jennifer, and me. We reminded the nurse that Margie had not been aggressive with the female staff of the facility.
It turns out that it was the inflexibility of the staff that prevented them from providing Margie with proper care.
Back to contents
Why do people with dementia experience violent attacks?
The principle of helping patients with agitation attacks can be formulated in a few words: adapt the environment, change the approach, treat medications last.
In our seminars for professional caregivers, we always repeat: if you are happy with the result, keep doing it! But if you don’t get a positive response as a result, then it’s time to try a different approach.
All types of behavior are a means of communication. When a person with dementia makes a scene, they are trying to tell you something.
Agitation often manifests itself as an inability to cope with stress, pain or overwork.
The most important thing is to find out whether the behavior is related to a specific event or is a reaction to an unusual environment that causes an emotional outburst that develops into an outbreak of aggression.
Behavior triggered by an event. For example, some unpleasant situation has occurred related to personal hygiene: the caregiver is trying to change the patient’s clothes after an incident of incontinence. A person with dementia may experience a stranger's intrusion into their personal space. Sometimes this evokes in the patient's memory some event in the past that was offensive to him.
Behavior provoked by the external environment. For example, a patient is transported from his home to a facility that closely resembles a hospital and becomes agitated. There is a possibility that the hospital atmosphere itself triggers the grief process in him, as it is associated with the loss of someone close.
Both of these types of memory stimulation—which generally have no negative consequences—can provoke unsightly, strange, or even dangerous behavior on the part of the person with dementia.
Pay attention to typical signs and even subtle hints that indicate that tension is growing. The sooner you manage to prevent an attack of agitation, the more effectively you will be able to correct the patient’s behavior.
Avoid direct prohibitions: don’t say “no” or “you can’t”, don’t try to physically prevent a person from doing something or going somewhere. The patient may perceive this as aggression and feel that he needs to defend himself.
Most often, anger attacks occur towards the end of the day, when stress and fatigue accumulate.
Back to contents
Consequences of behavior disorder
Behavioral symptoms develop at any stage of the disease. Typically, several manifestations belonging to one or more clusters occur simultaneously.
Thus, with aggressive behavior, the patient becomes unfriendly and may push away, hit, or curse. Aggression is often accompanied by agitation (the patient is agitated and fussy).
If the disorder manifests itself as psychosis, then the patient watches those around him on the sly or follows on his heels. When agitated, he may try to leave the house or sit, constantly smoothing his hair, rubbing the skin of his face in one place, or trying to remove a sore, sometimes tearing it until it bleeds.
The consequences of untreated symptoms can be:
- For the sick. Decreased quality of life, increased dementia, and the emergence of additional risks to life.
- For relatives. Deterioration of financial situation, lack of time, lack of personal interests and increased risk of depression.
At the same time, the patient may exhibit different clusters of symptoms, as well as manifestations of mental and cognitive personality destruction.
Reasons for increased behavioral symptoms
If the patient is unable to provide safety, adequate medical care and a friendly environment, then dementia will worsen. Lack of care provokes an increase in the symptoms of the disease, leading to inappropriate behavior when the ward spits, screams, displays increased sexuality, unfriendliness, and aggression.
Increasing frustration is accompanied by swallowing objects, the disappearance of the difference between day and night in the patient, and stubborn refusal to help.
Contribute to increased symptoms:
- Pain caused by injury or illness.
- Change of residence.
- Changing nursing staff in a nursing home or home.
- Deterioration of vision or hearing.
- The actions of others are misinterpreted and taken as a threat.
- Bathing.
- Travel, long trip.
- Irritation when performing normal activities (dressing, eating)
Apathy and depression contribute to separation from reality and loss of desires. The patient in this state refuses to eat, sleeps poorly, and is not interested in his usual hobbies.
Approximate diet of a patient with dementia
To ensure that the balance of all nutrients is maintained, it is recommended to create a menu that includes all the necessary products.
An approximate diet for a patient with dementia for one day is presented in the table below. Nutrition menu for a patient with dementia for one day
| Meal time | For a patient who is able to swallow solid food | For a patient with impaired swallowing |
| Breakfast |
|
|
| Lunch |
|
|
| Dinner |
|
|
| Afternoon snack |
|
|
| Dinner |
|
|
Important! The menu should be adapted to concomitant diseases.
When is hospitalization required?
The disease, regardless of the cause of its occurrence, progresses over time. If left untreated, it inevitably leads to a complete loss of human independence. To avoid missing early signs of developing dementia, all people over 65 should be screened for dementia risk at least once a year.
Increasing dementia of the ward leads to a stressful load on others. Not understanding the nature of the disease, they are not always able to ensure the safety of a relative.
If behavioral disorders are left untreated, the development of severe dementia accelerates. At the stage of severe dementia, the patient requires qualified nursing care, for which he is admitted to the hospital.
Behavioral manifestations of the disease negatively affect the patient’s condition and the mental health of those caring for him.
The family bears a heavy burden of emotional, time and material costs. With insufficient care for the ward, increased depression, agitation, and the appearance of delusional ideas, the likelihood of causing harm to oneself (suicide) or others increases (due to forgetfulness, I forgot to turn off the water, turn off the gas, turn off the iron).
Read our article about security systems for the elderly.
A patient in this condition should be cared for by qualified nursing home health workers who are trained to deal with any manifestations of the disease. With severe aggression, directed at other people or at oneself, it may be necessary to place the patient in a psychiatric clinic.
Algorithm for correction of behavioral symptoms of dementia
To reduce the behavioral manifestations of dementia, special non-pharmacological strategies are used. This is necessary to reduce the drug load on the body of older people, who usually suffer from several chronic diseases and take many pills.
Non-pharmacological approaches can ensure satisfactory well-being of the patient, mitigate the negative manifestations of the disease, and improve the quality of life.
For each specific case, the approach to identifying and correcting the problem will be different, but in general, the methods for eliminating this problem are similar. American researchers L.N. Gitlin and H.S. Kales propose an algorithm for correcting behavioral symptoms of dementia. Correction of violations is carried out in 6 stages.
What should a diet for dementia include?
Products for dementia should be selected in such a way as to reduce the level of exposure to the main causes leading to the disease. This is what primarily affects the patient’s body:
- Accumulation of a large number of free radicals. Their elimination is ensured by antioxidants, which are found in nuts, citrus fruits, green vegetables, and seafood.
- Atrophic changes in tissues. Vitamins for dementia, primarily A, C, E, can somewhat slow down this process. Therefore, they should be present in the daily diet, not only in the form of food, but also as multivitamin preparations.
- Blockage of blood vessels and subsequent oxygen starvation of tissues. This is usually due to the accumulation of cholesterol, so foods that lower it will help improve the condition. Legumes, blueberries, avocados, and vegetable oils will come to the rescue.
- Dehydration of tissues. The easiest way is to avoid it. To do this, it is enough for the patient to drink a sufficient amount of clean water.
Important! Simply consuming the listed products is not enough. Their quantity must be balanced in the diet.
Stage 1: Identify the problem
At the first stage, the problem is identified and preventive measures are taken. Screening is required to prevent dementia from rapidly worsening.
Screening is carried out independently, using self-monitoring tests, or by visiting a psychiatrist. A visit to the doctor is required if testing reveals behavioral, cognitive or mental abnormalities.
If screening results are positive indicating an increased risk of dementia, assess:
- Patient's health.
- The nature of family relationships.
- The quality of care that the family is able to provide.
- Adequate sleep and diet.
- The patient's ability to recognize the problem and take care of himself.
The health of a person suffering from a brain disorder depends on the quality of care and the correct behavior of family members. The more people around you know about the disease, the better they can care for a relative with dementia.
Stage 2. Characteristics of the behavioral problem
Having assessed the general condition of the patient at the first stage of diagnosis, we move on to identifying a specific symptom that requires correction. Any, even minor, change in behavior requires a professional assessment by a psychiatrist.
See also:
- Dementia stages and disease prognosis: challenges and solutions along the disease trajectory
- 13 Online Dementia Tests: Check Your Brain Health
- Leg pain in older people: possible causes and treatment
To prevent accelerated progression of dementia, you should:
- Discuss the manifestations of the disease with your doctor.
- Determine the nature of the behavior disorder. This is necessary to develop the right plan of action.
- Talk to the patient. At the first stages, he is able to assess his own behavior, his level of deviation from the norm.
- Draw up an action plan. Consider the level of care (home or hospital placement), determine the risks for the patient.
The conversation with the patient includes questions to determine which category of behavioral symptoms the existing deviations in the patient’s behavior should be classified into.
Sample questions to determine the nature of behavioral manifestations:
- What does the patient consider wrong in his behavior?
- Why is this behavior a violation?
- In what cases does the disorder occur?
- At what time of day or day of the week does the violation occur?
- Where does the violation occur?
- What event preceded the onset of the symptom?
- How did others react to the event?
- What accompanied the manifestation (the TV was on, people were present)?
- How do you think the problem can be dealt with?
At stage 2, the most common manifestations of behavioral disorders are identified, the level of stress in the patient and family members is determined, and how correctly he can assess his condition is determined.
Causes of constipation in old age
Age-related changes affect all organ systems. The intestines are no exception, the motor activity of which decreases significantly in old age. Other reasons for the development of constipation include the following:
- Low water consumption;
- Incorrect diet;
- Lack of physical activity;
- Some diseases (diabetes, atherosclerosis and others);
- Use of certain medications.
The process of treating constipation in an elderly person must be carried out under the supervision of specialists, which will allow timely identification and elimination of emerging problems.
Stage 3. Identifying the causes of behavioral disorder
There are no medications that can reverse dementia. We have not yet learned how to completely cure this disease. But those around you can influence the well-being and mood of the ward by improving his living conditions, changing his daily routine, and learning to recognize his needs and desires.
Three groups of factors can cause or intensify behavioral disorders:
- medical care;
- features of life;
- type of care (nursing, nursing home).
Health problems that frequently arise with dementia require medical correction:
- dehydration;
- insomnia;
- pain;
- increased risk of falls.
When communicating with people with moderate to severe dementia, be aware that they may not be able to communicate a medical problem or the source of their body pain. It is imperative to ask patients in detail:
- How often do they go to the toilet to find out if they have diarrhea, constipation, cystitis or prostatitis.
- Do they feel anxious?
- Do they have fears to identify possible delusional disorders?
- Do they experience disorientation in space and time?
If the ward is at home, then his living conditions should be analyzed. In everyday life, the manifestations of dementia can increase:
- increased noise level;
- room illumination (lack of lighting or excessively harsh light);
- clutter in the house (difficult to find the things you need);
- temperature and humidity in the room;
- cramped conditions, clutter of furniture in the house;
- large family, crowded living.
A large number of people, excessively bright lighting, noise, disorder and other stimulating external factors cause anxiety and agitation in the patient, and increase the progress of the disease.
The absence or lack of stimulating factors has a negative effect. Poor lighting, lack of communication, lack of music to listen to, or TV shows leads to apathy, which accelerates the process of personality destruction.
Factors that contribute to increased behavioral disorders include the nature of communication between the ward and caregivers. It is necessary to analyze how the caring staff or the patient’s relatives communicate with him.
If the caregiver is impatient, speaks loudly and in a harsh tone, this causes a negative reaction in the patient. He can:
- resist leaving;
- refuse to wash;
- try to leave the house.
Patients are extremely sensitive to the emotional tone of voices and the mood of others. If signs of aggressive behavior appear in the ward's behavior, the caregiver needs to analyze:
- How to communicate with a patient so as not to provoke agitation.
- Can a rush or an unplanned procedure become a source of violation.
- How professionally is the caregiver able to control his mood and maintain a friendly tone.
How to prevent it?
You can reduce aggression by listening to calming music or playing musical instruments. A patient suffering from dementia often becomes aggressive when bathing or changing clothes. Therefore, it is recommended to turn on relaxing music in advance before starting hygiene procedures.
It is recommended to eliminate the following factors that complicate the patient’s life:
- Lack of light in the room.
- Fever.
- Having difficulty finding a toilet.
You can stick appropriate inscriptions on furniture and kitchen appliances. To reduce the manifestation of aggression in senile dementia, perform physical exercises. Physical activity helps improve sleep and eliminate negative emotions. You can invite the patient to spend the evening in the company of family or relatives to awaken positive memories.
Stage 4. Drawing up a plan for correcting behavioral symptoms
At the 4th stage of treatment, the disorder actually draws up an action plan. It should include:
- Generalized goals specific to all types and stages of the disease.
- Solving an individual problem.
- Selecting specialists for medical consultation.
Goals common to all types of dementia include scheduling procedures, daily routines, and performing them accurately. The structure of the day and the predictability of actions help the ward to maintain contact with the world, and actions acquire meaning.
An example of a generalized approach is improving education and support for caregivers, their skills and overall well-being. This approach reflects good integrated dementia care practice that can prevent or reduce behavioral symptoms.
Listening to music is considered promising for dementia. It has been established that musical abilities remain in most people into old age.
Under the influence of music, there is a decrease in aggressiveness and agitation. Patients who regularly listen to their favorite pieces of music are less prone to wandering, fussiness, and repetitive gestures.
To solve a specific problem, all possible factors influencing the situation are considered. If, for example, a person complains that he hears voices, he should:
- evaluate hearing;
- select or adjust a hearing aid;
- Check the functionality of the hearing aid.
It is possible that auditory hallucinations are caused by poor hearing, which forces the person with dementia to listen intently. This increases excitement and activates conjecture and imagination, which, in turn, gives rise to fear.
If the patient is afraid to fall asleep in the dark, a night light is placed at the head of the bed. When complaining of poor sleep, check how comfortable the sleeping conditions are, whether the patient drinks drinks containing caffeine at night, and whether he sleeps too much during the daytime.
The strategy for non-drug treatment of depression necessarily includes visits by caregivers to specialists in psychology and gerontopsychology, occupational therapy and nursing care. They must teach caring staff how to respond to the behavior of the ward, explain what needs to be done to improve the life of the patient himself and the family as a whole.
Example of a targeted non-pharmacological strategy
Statistics show the relevance of dementia treatment. Due to increasing life expectancy and the aging of the planet's population, the incidence of the disease is growing, and by 2050, according to WHO forecast, it will reach 115.4 million people.
In addition to the patients themselves, dementia becomes a serious problem for family members. Treatment lasts for years, requires a lot of effort from those around you, leaves no free time, and increases material costs.
For example, a 93-year-old man who suffered from mild cognitive impairment at the onset of his illness had a dementia test on the MMSE of 29 out of 30 possible points. After 6 years, the test result dropped to 21 out of 30, and behavioral disorders joined cognitive impairment.
The man began to hear noises and voices at night, which disturbed his sleep, and during the day he slept a lot and was in a depressed mood. Another year later, the patient left the house, lost orientation in space and got lost.
As a result, the man was taken by ambulance to the hospital, where he was prescribed non-drug correction:
- Forgetfulness. Use a calendar, medication schedule, pill dispenser.
- "Voices" and noise at night. Select a hearing aid, identify possible sources of noise (working TV, cat, clock striking).
- Insomnia. Increase physical activity during the day, eliminate bright lighting and violent emotions in the evening.
Physical activity means performing feasible active and passive gymnastics, walking, and caring for plants in the garden. It is useful at all stages of dementia to communicate with pets and observe their behavior.
During the examination, the psychiatrist necessarily excludes the possibility of taking medications and the possibility of other diseases. When examining a patient, the doctor must also rule out depression, an infectious disease, trauma or other internal disease, and determine what level of care the patient requires to mitigate the manifestations of the disease.
| Comparative characteristics of depression and dementia (according to LGCohen, 1999) | ||
| Mental state parameters | Depression | Dementia |
| Affect | Depressive | With irritability and outbursts of rudeness |
| Worsening | Labile, losing nuances | |
| Significant subjective distress | Lack of subjective concern about one’s condition | |
| Start | Fast | Gradual |
| Can be precisely dated | Time estimate is uncertain | |
| History of depression and other mental disorders | The disorder manifests itself for the first time | |
| Flow | Short duration of symptoms before seeking medical help | Long-term course until seeking medical help |
| Rapid increase in symptoms after onset | Slow development of symptoms over time | |
| Behavior | With a predominance of indifference, inability to react | With a predominance of distractibility, preoccupation |
| Passivity: any action requires effort | Fussiness: “struggle” to perform an action | |
| There are no attempts to compensate for the failure | The desire to compensate for failure with memorial notes | |
| Persistent and often complete loss of social contacts | Social contacts are relatively intact | |
| Behavior not consistent with severe cognitive dysfunction | Behavior comparable to severity of cognitive dysfunction | |
| Increased dysfunction in the evening and night hours is not typical | Dysfunction often increases in the evening and night hours | |
| Complaints | Multiple complaints of cognitive impairment | Isolated complaints of cognitive impairment or lack thereof |
Step 6: Monitoring the symptom management regimen
At the sixth stage, constant monitoring of the patient’s condition is carried out, the appearance of new symptoms that arise during the development of the disease is monitored. The accepted scheme for the correction of symptoms of dementia also includes the assessment of comprehensive care, including the correction of cognitive impairment and mental disorders.
Behavioral symptoms are not constant, and as the disease progresses, they appear suddenly and then disappear just as suddenly. The task of caregivers caring for the patient is to notice new signs of the disease in a timely manner and include them in the overall behavior correction scheme.
It is necessary to monitor behavioral disturbances, as well as factors that contribute to the worsening of the disease. Thus, with aggression provoked by unfriendly communication, cognitive disorders (forgetfulness, difficulty speaking, memory impairment) may temporarily increase.
Non-drug methods for correcting behavioral symptoms are not always able to fully compensate for the patient’s condition. If the effectiveness of non-pharmacological strategies is low, the patient is provided with professional nursing care at home or in a hospital, and drug therapy is prescribed.
Generalization
The approach to managing symptoms of dementia must be multi-component. The proposed 6-step algorithm is a guide for doctors, nursing staff and relatives caring for a person with dementia.
The method allows you to assess the degree of dementia, identify the nature of the disorders and select an appropriate treatment regimen for the disease, without immediately resorting to prescribing medications. A non-pharmacological approach to the treatment of behavioral symptoms of dementia allows the patient to maintain satisfactory health for a long time and delays the time of hospitalization in a nursing home or psychiatric clinic.