What is ataxia?
Ataxia comes from the Greek word ἀταξία meaning “irregularity” or “disorder,” but in medical usage the term describes a condition characterized by poor coordination of movements. Ataxia can cause involuntary eye movements (nystagmus), poor hand coordination, difficulty with fine motor skills (such as eating or writing), difficulty speaking, and unsteady walking. This can make a person appear "drunk."
Patients with ataxia cannot walk in a straight line and tend to bump into things. In advanced stages, they may need a walker or even a wheelchair. Patients may also have vision problems due to eye movement disorders. Damage or degeneration in the back of the brain, called the cerebellum, results in ataxia. The disorder may also occur due to problems with the sensory system (abnormal perception of the position of a body part in space) and the vestibular system (abnormal balance). A neurologist usually distinguishes two types of ataxia: motor and sensory.
Causes of the disease
A person can get Friedreich's ataxia only if both of his parents are carriers of the pathologically altered gene. The mutation occurs in the long arm of chromosome 9 , which provokes pathologies during the formation of the protein frataxin from mitochondria, which plays the role of “energy cell stations.”
Iron accumulates in mitochondria, which is then oxidized. Oxygen is transported in the body. When iron synthesis is disrupted, its volume in mitochondria increases significantly and sharply (approximately tens of times). Moreover, cellular iron is within normal limits, and the amount of cytosolic iron decreases.
These processes activate genes encoding fragments that are responsible for the delivery of iron - permeases and ferroxidases. Thus, the balance of intracellular iron is further disrupted. Due to the increased concentration of iron in the cell, radicals are activated, which have damaging properties and destroy the cell from the inside . The most vulnerable cells are neurons (especially in the fibers of peripheral nerves, in the spinocerebellar tracts, lateral and posterior columns of the spinal cord).
Taking into account the degree of gene mutation, “classical” types of disease are distinguished from atypical diseases, so to speak, benign syndromes, lighter versions.
Friedreich's hereditary ataxia is the most common of all types of ataxia.
Signs and symptoms
Symptoms of ataxia vary depending on the person and the type of disorder. The rate of progression also varies. Symptoms may worsen slowly over decades—or quickly over months. General symptoms of ataxia:
- lack of coordination;
- slurred speech;
- problems with eating and swallowing;
- deterioration of fine motor skills;
- difficulty walking;
- gait abnormalities;
- eye movement disorders;
- heart problems.
People with ataxia often require the use of wheelchairs and walkers to get around.
Diagnostic methods
To diagnose the disease, a neurologist collects a family history.
Conducts neurological tests and functional tests (Romberg test, tandem walking). This allows you to see the picture of symptoms in more detail. Instrumental diagnostics include:
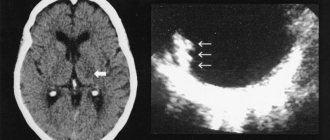
- CT, MRI of the brain;
- electroneuromyography;
- EEG;
- duplex scanning of cerebral vessels;
- biochemical and general blood test;
- genetic analysis.
The neurologist can refer you for consultation to an otolaryngologist and neurosurgeon if necessary.
Causes and types
There are many causes of ataxia, but most can be categorized as sporadic (no specific cause), genetic (also called hereditary or familial), or secondary to medical conditions, certain medications, or brain damage.
Congenital ataxias occur in children and are most often caused by structural abnormalities in the brain that occur before or during birth. These include cerebral palsy (often associated with damage to the brain at birth due to lack of oxygen or blood supply), hydrocephalus (high blood pressure caused by a blockage or buildup of cerebrospinal fluid), brain tumors, and other brain injuries.
Ataxia may occur suddenly (acute), over a period of weeks (subacute), or progress slowly over months or years (chronic). In acute cases, the most common cause is a stroke or hemorrhage in or around the cerebellum. Patients typically present with headache, vomiting, neck stiffness, or loss of consciousness. In children, bacterial or viral infections can cause acute ataxia, which usually resolves with time. They develop a fever, trouble walking, and slurred speech within hours or days, and recover within a few weeks. Subacute onset of ataxia is usually observed in paraneoplastic cerebellar degeneration. This is a condition in which breast cancer, lung cancer, ovarian cancer, or other areas of the body produce antibodies that affect the cerebellum and cause the disorder.
LiveInternetLiveInternet
Cattus_13
all posts by the author
Ataxia
(Greek ἀταξία - disorder) - impaired coordination of movements; one of the most commonly observed motor disorders.
There are static ataxia (impaired balance when standing) and dynamic ataxia (discoordination during movements).
Types of ataxias in clinical practice:
- sensitive or posterior columnar (ataxia due to disruption of the conductors of deep muscle sensitivity);
- cerebellar (ataxia with damage to the cerebellum);
- vestibular (ataxia with damage to the vestibular apparatus);
- cortical (ataxia with damage to the cortex of the frontal or temporo-occipital region).
Now point by point.
I. Sensitive ataxia
- specific disturbance of gait and coordination of movements. Occurs when there is a violation of the muscular-articular sense, which, in turn, can occur when there is damage to:
- posterior columns of the spinal cord (they represent a powerful system of fibers of various origins; in terrestrial mammals, they are formed in evolution in connection with the development of the limbs, when the need arises for a subtle analysis of information from the joints and skin, without which walking, running, jumping, maintaining balance and body position in space.);
- spinal nerves (transmitting afferentation from the receptor apparatus of the limbs);
- thalamus (receiving in its ventrobasal part the axons of neurons of the pathways);
- peripheral nerves (for polyneuropathy).
When the above formations are damaged, a person ceases to feel support, which, in the absence of visual control or in conditions of insufficient lighting, becomes quite critical for assessing the position and movement of the body in space. The gait becomes “stamped”. The patient “stamps” each step to be sure that the foot is on a hard surface. (A similar feeling is if, while climbing the stairs, you think that there should be a step under your foot, you take a step and “fall through”, slamming your foot into the floor.)
II. Cerebellar ataxia is a general term indicating a lack of coordination of movements due to damage or diseases of the cerebellum and its connections. It manifests itself as specific disturbances in gait (cerebellar dysbasia), balance, incoordination of movements, impaired speech fluency (cerebellar dysarthria), various types of cerebellar tremor, muscle hypotonia, oculomotor dysfunction and, sometimes, dizziness. Due to the many different types of cerebellar lesions and the clinical diversity of the described symptoms, a unified classification of cerebellar ataxia has not been created to this day. For a practicing neurologist, a classification based on clinical signs and features of the course of ataxia is convenient, greatly facilitating the diagnostic search.
Ataxia with acute onset:
- Vascular accidents, or space-occupying formations with a pseudo-stroke course
- Multiple sclerosis
- Guillain-Barre syndrome
- Post-infectious cerebellitis and encephalitis
- Intoxication (including drugs - lithium preparations, barbiturates, diphenine)
- Metabolic disorders
- Hyperthermia
- Obstructive hydrocephalus
Ataxia with subacute onset (one to several weeks):
- Abscesses, tumors and other space-occupying processes in the cerebellum
- Normal pressure hydrocephalus
- Toxic and metabolic disorders (including disorders of nutrition and nutrient absorption)
- Paraneoplastic cerebellar degeneration
- Multiple sclerosis
Chronic progressive ataxia:
- Spinocerebellar ataxias (early onset)
- Cortical cerebellar ataxias
- Late-onset cerebellar ataxias involving the brainstem and other parts of the nervous system
Paroxysmal episodic ataxia
In children: autosomal dominant hereditary periodic ataxia (two types, depending on the duration of the attacks) and other ataxias (maple syrup disease, Hartnup disease, pyruvate dehydrogenase deficiency)
In adults, episodic ataxia is most often caused by transient ischemic attacks, drugs, multiple sclerosis, volumetric compression in the foramen magnum, intermittent obstruction of the ventricular system
(you can read more about all types of cerebellar ataxia, for example, in V.L. Golubev and A.M. Wayne in the fundamental work “Neurological Syndromes”; perhaps we will return to the description of individual causes of ataxia later)
III. Vestibular ataxia
(or “labyrinthine”, according to some authors) is a specific disorder of gait and coordination of movements that develops when one of the sections of the vestibular apparatus is damaged - the labyrinth, vestibular nerve, nuclei in the brain stem and the cortical center in the temporal lobe of the brain. Ataxia itself is complemented by a clinical picture of damage to the vestibular apparatus: systemic dizziness (it seems to the patient that all objects around him are moving in the same direction), when turning, with sudden movements of the head or changes in body position, this dizziness intensifies. In this regard, the patient staggers randomly or falls, and makes head movements with noticeable caution, which is accompanied by nausea and vomiting. This also includes horizontal nystagmus and possible hearing impairment. Vestibular ataxia is observed in brainstem encephalitis, ear diseases, tumors of the fourth ventricle of the brain, as well as in Meniere's syndrome. In fact, this syndrome can be considered a specific subtype of sensitive ataxia. Patients with vestibular ataxia demonstrate gross impairment of walking and standing (vestibular balance disorder), but without involvement of the limbs or speech. With unilateral lesions of the labyrinth, the “flanking gait” in the direction of damage is significantly impaired.
IV. Cortical atxia (“frontal”) - its development is caused by damage to the frontal lobe of the brain caused by dysfunction of the fronto-pontine-cerebellar system. In frontal ataxia, the leg contralateral to the affected cerebellar hemisphere is most affected. When walking, instability is observed (more so when turning), tilting or leaning towards the side ipsilateral (i.e. corresponding to the same side) to the affected hemisphere. With severe lesions of the frontal lobe, patients cannot walk or stand at all. Vision control has no effect on the severity of walking disorders. Cortical ataxia is also characterized by other symptoms characteristic of damage to the frontal lobe - the grasping reflex, mental changes, and impaired sense of smell. The symptom complex of frontal ataxia is very similar to cerebellar ataxia. The main difference between cerebellar lesions is evidence of hypotonia in the ataxic limb. Common causes of frontal ataxia are cerebrovascular accidents, abscesses, and tumors.
A little about diagnostics.
Anamnesis. A carefully collected medical history makes up a large part of the diagnosis. According to anamnestic data, it is possible to divide developed ataxia (see classification above) into acute, ataxia with subacute onset and chronic, episodic, from here the diagnostic search will proceed according to nosoological units. Sensitive ataxia - manifests itself with loss of visual control, this is a specific symptom. With vestibular ataxia, it is also more or less clear, signs of damage to the vestibular apparatus in combination with medical history, consultation with an ENT doctor (if you find it difficult to independently assess the damage). In other cases, difficulties arise, and then in patients with ataxic disorders, the diagnosis is based primarily on neuroimaging (CT, MRI) and neurophysiological (evoked potentials, electroneuromyography, etc.) studies that provide data on the structural and functional characteristics of the central and peripheral nervous system. systems. In most cases of hereditary ataxia, verification of the diagnosis using DNA analysis is now available both for the patients themselves and for their clinically healthy relatives from the “risk” group. To prevent new cases of the disease in these families, medical genetic counseling and prenatal DNA diagnostics can be carried out. In patients with sporadic ataxia, it is necessary to search for all possible somatic disorders that can cause cerebellar symptoms (neoplasms, endocrine diseases, etc.). Ataxia can be a manifestation of a number of metabolic diseases, so appropriate biochemical screening should be carried out.
In the neurological status, we must pay attention not only to the coordinating sphere (In the Romberg position, it is stable or deviates to the right/left/back/forward (with open and closed eyes). Performing the finger-nose test, knee-heel test satisfactorily or with intention tremor, m. b. missed hit. Test for hitting the hammer. Tests for dysdiadochokinesis, dysmetria (test of lowering the arms, pronation test, reverse push symptom - Stewart-Holmes symptom). Scanned speech. Gait with open and closed eyes.), neurological status data should be Pay close attention to the whole - focal signs, pathological symptoms - all this together will push us to determine the level of damage, and, subsequently, to the cause.
By the way, I almost forgot. Psychogenic or hysterical ataxia presents with bizarre changes in walking: the patient can move as if he were a speed skater, walk along a broken line, cross his legs when walking, or move on straightened legs, as if on stilts. This kind of ataxia often occurs in combination with other functional or even some organic disorders. This type of movement disorder is exclusively functional, and a judgment about psychogenic ataxia is appropriate if an objective examination and data from additional methods do not provide a convincing judgment about the genesis of the disease. In case of functional impairment, we always pay attention to the following points:
- the abundance and colorfulness of the described complaints (this point is typical for all “functional” patients, due to personal characteristics and the significance of the disease for the patient’s personality)
- discrepancy between the number of complaints and the severity of the patient’s condition
- connection between the onset of the disease and a psychotraumatic situation (death or loss of a significant person, troubles at work, significant difficulties in the social sphere in which going into illness is, although not a conscious, but “positive” way out of a difficult situation)
- often a unique clinical picture, causing difficulties in differential diagnosis
- the patient has a secondary medical education or a place of work related to medicine, combined with personal characteristics (the desire to “try on the disease” for oneself)
- multiple hospitalizations/examinations with a large number of diagnoses (sometimes with a large number of surgical interventions in a short period
- “beautiful indifference” - with all the “severity” of what is being described, the patient smiles or laughs while talking about his misadventures
Treatment
Of all movement disorders, ataxia is one of the most resistant to medical therapy. Clonazepam may help with tremors and balance problems. However, it has side effects such as sedation, fatigue or loss of libido, among others. Other medications such as buspirone or 5-hydroxytryptophan have been studied but have not been shown to be very helpful. Phenytoin, an anticonvulsant drug, is useful in some episodic ataxias. Acetazolamide is also useful in some rare forms of episodic ataxia.
Space and the cerebellum
The cerebellum is a small organ located at the back, under the occipital lobes of the brain. It is small in size. However, it is he who is responsible for the coordinated chain of needs and consequences for performing certain actions, both individual parts of the dynamic chain and their totality.
This part of the brain develops faster than all others in the first year of life, because it is during this period that children learn to sit, stand and walk, use their hands to grasp and hold objects, and learn to coordinate their actions in accordance with need.
The cerebellum itself is a complex system consisting of several components. One of them has a very unusual name - a worm. It is responsible for the balance of the body, its tone, posture, and supporting movements. Disturbances in the functioning of this part of the cerebellum lead to a syndrome called cerebellar ataxia. The static and dynamic forms of such a disorder depend on its manifestation in movements or rest. Be careful.
Forecast
The prognosis of the disease can vary significantly and depends largely on the type of disorder. Some types may remain relatively stable or even improve over time, but most will gradually get worse over many years.
Life expectancy is generally shorter than usual for people with hereditary ataxia, although some people may live into their 50s, 60s, and beyond. In more severe cases, the condition can be fatal in childhood or early adulthood.
For acquired ataxia, the prognosis depends on the underlying cause. Some cases may improve or remain the same, while other cases may gradually worsen over time and shorten life expectancy.
Disease prognosis
Friedreich's ataxia has an inevitably progressive course, which ends in the death of a person due to cardiac or respiratory failure. Half of sick people do not live to be 40-45 years old. There have been cases where the patient managed to live up to 70 years. This can happen in the absence of diabetes and heart disease. Therefore, if possible , it is necessary to avoid having children when there have been cases of Friedreich's ataxia in the family, and you should not marry between relatives.