Svetlana Shcherbakova
Cardiologist
Higher education:
Cardiologist
Kabardino-Balkarian State University named after. HM. Berbekova, Faculty of Medicine (KBSU) Level of education – Specialist 1994-2000
Additional education:
“Cardiology”
State Educational Institution “Institute for Advanced Training of Physicians” of the Ministry of Health and Social Development of Chuvashia
Contacts
Medical statistics place stroke in one of the first places in the world as a cause of disability. Only 20% of patients who have undergone it return to a full life. These are mostly people of working age. For older people, it ends with the loss of some body functions and the loss of the ability to self-care. Doctors are sounding the alarm - acute cerebrovascular accidents are increasingly occurring at a young age. Therefore, it is so important to develop effective rehabilitation individually for each patient. This requires an objective assessment of the patient’s functional state after a stroke.
Assessment of the patient's condition after a stroke
To assess the patient's neurological condition, various scales are used, based on clinical examinations of reflexes and functional tests. They allow you to evaluate the effectiveness of the treatment and draw up a rehabilitation plan. The Rankin scale allows you to determine the degree of disability after a stroke. Disability is a consequence (outcome) of severe brain damage, in particular stroke, which entails impairment of motor activity, sensitivity, cognitive functions and the emotional sphere.
Neurologists have been using the Rankin Scale since 1988. In its initial form, it included 6 steps - from zero (no consequences) to 6 - death of the patient. The subsequently created modified scale is intended specifically to establish the level of loss of vital functions for the development of further rehabilitation of the patient.
Rating scales
The Rankin Scale involves the use of data obtained as a result of examining the neurological condition of a patient with a stroke using the NIHSS scale developed by the American National Institutes of Health. It establishes a scoring system from minimum values - 3 - 5 points to 25. Tests are used not only to determine the severity of a stroke, but also to plan further treatment (thrombolytic therapy). The scale allows you to evaluate:
- level of speech preservation;
- pain sensitivity;
- degree of motor dysfunction;
- ability to concentrate;
- level of consciousness;
- level of coordination of movements.
Another rating system is the Barthel scale. It makes it possible to determine the degree of dependence of the patient on outside help. The assessment criteria are the ability to perform everyday activities:
- all personal hygiene procedures (washing, bathing, brushing teeth, shaving);
- eating food, including the ability to cut it;
- dressing;
- going to the toilet;
- movement (getting out of bed, range of independent movement, climbing stairs).
Bringing together the indicators of the tests and examinations performed, the doctor analyzes the data and assigns the patient the appropriate level on the Rankin scale.
Diagnostics
Diagnosis of derealization consists of interviewing the patient and determining its clinical manifestations using the Nuller scale. The study is conducted by a psychiatrist. Laboratory and instrumental tests are prescribed (clinical blood test, clinical urine test, MRI, ultrasound examination of the head).
Criteria for diagnosing derealization:
- The patient complains of a feeling of unreality of the world around him, that objects or objects have become unrecognizable.
- A critical assessment of their own thoughts and state is maintained, they understand that this state appears suddenly, that only they feel or see it.
- The patient is clearly conscious.
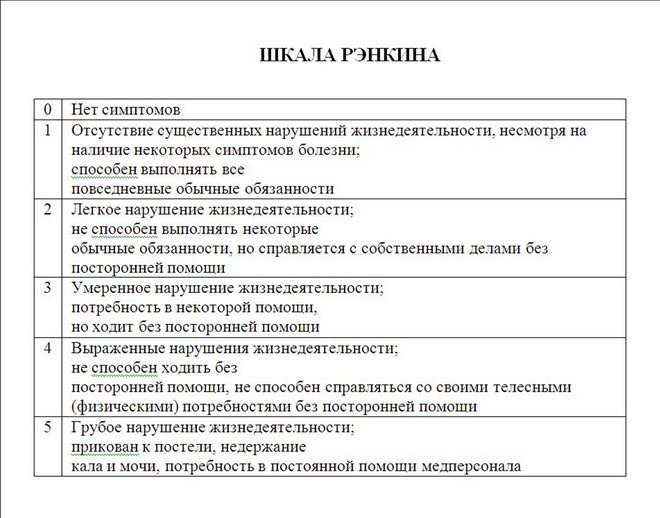
Rankin scale
Its principle is the division of dysfunctions according to the level of severity. Zero degree is the easiest, fifth is the most severe, when a person will not be able to recover from the consequences of a stroke for life:
- Zero – no violations.
- 1st degree. Capacity is slightly reduced, the patient can perform all the usual actions. Minor impairments may affect speech, reading and writing. These may include emotional disturbances, decreased sensitivity, and difficulty moving. At the same time, he retains the ability to perform work, move independently and do ordinary things. The word “ordinary” means actions that he performed more than once a month.
- 2nd degree – moderate (mild) loss of capacity. At this degree, the ability to self-care is preserved, but the ability to do ordinary things is lost. These include driving, working, reading and others. At the same time, a person can independently take short walks, go to the store, and cook food. Grade 2 loss of capacity assumes that the patient can remain without outside help for more than one week.
- 3rd degree – average loss of capacity. Such a patient needs outside help for housekeeping - going to the store, preparing food, and cleaning the house. At the same time, he is able to independently move around the apartment, perform natural necessities, and perform daily toileting. Such patients require supervision several times a week. Some of them need psychological help.
- 4th degree. Moderate-severe incapacity requires the presence of an assistant in the home every day. In this condition, the patient cannot move without assistance and take care of himself. But he can be left alone for a short time. It is possible to distinguish between degrees 4 and 5 precisely by this indicator - how much time during the day the patient can spend alone.
- Grade 5 – severe. The person is bedridden, has urinary incontinence, and needs a permanent caregiver.
Rehabilitation is the main component of medical care after treatment of an acute condition due to stroke. This is a long process aimed at getting rid of neurological disorders as much as possible. The success of rehabilitation treatment largely depends on the individual characteristics of the patient. The Rankin scale greatly simplifies the task of the neurologist, who must draw up a step-by-step rehabilitation plan. In addition, these scales also help doctors who directly carry out measures to restore the patient. It is also used in the rehabilitation process itself to evaluate its effectiveness.
The scale also allows you to determine the need to use and the type of mobility aids (cane, walker, stroller).
Taylor test. Anxiety scale rating
Taylor test
| Full name of the person being assessed | ____________________________________________ |
| Age (full years) | ____________________________________________ |
| Job title | ____________________________________________ |
| Subdivision | ____________________________________________ |
| Date of completion | ____________________________________________ |
Instructions
Please put “yes” next to those provisions with which you agree, and “no” – next to those with which you do not agree.
Test
| № | Question | Answer | |
| Yes | No | ||
| 1 | I can work for a long time without getting tired | ||
| 2 | I always keep my promises, regardless of whether it is convenient for me or not. | ||
| 3 | My hands and feet are usually warm | ||
| 4 | I rarely have a headache | ||
| 5 | I'm confident in my abilities | ||
| 6 | Waiting makes me nervous | ||
| 7 | Sometimes I feel like I'm good for nothing | ||
| 8 | I usually feel quite happy | ||
| 9 | I can't concentrate on one thing | ||
| 10 | As a child, I always immediately and resignedly carried out everything that was assigned to me. | ||
| 11 | Once a month or more often I have an upset stomach | ||
| 12 | I often find myself worrying about something | ||
| 13 | I think I'm no more nervous than most people | ||
| 14 | I'm not too shy | ||
| 15 | Life for me is almost always associated with a lot of stress | ||
| 16 | Sometimes it happens that I talk about things that I don't understand | ||
| 17 | I don't blush more often than others | ||
| 18 | I often get upset over small things | ||
| 19 | I rarely notice my heart palpitations or shortness of breath | ||
| 20 | I don't like all the people I know | ||
| 21 | I can't sleep if something is bothering me | ||
| 22 | I'm usually calm and not easily upset | ||
| 23 | I often have nightmares | ||
| 24 | I tend to take things too seriously | ||
| 25 | When I'm nervous, I sweat more | ||
| 26 | I have restless and interrupted sleep | ||
| 27 | In games I prefer to win rather than lose. | ||
| 28 | I'm more sensitive than most people | ||
| 29 | It happens that indiscreet jokes and witticisms make me laugh | ||
| 30 | I would like to be as happy with my life as others probably are | ||
| 31 | My stomach is bothering me a lot | ||
| 32 | I am constantly preoccupied with my material and official affairs | ||
| 33 | I am wary of some people, although I know that they cannot harm me | ||
| 34 | Sometimes it seems to me that difficulties are piled up in front of me that I cannot overcome | ||
| 35 | I get confused easily | ||
| 36 | At times I become so excited that it prevents me from falling asleep | ||
| 37 | I prefer to avoid conflicts and difficult situations | ||
| 38 | I have attacks of nausea and vomiting | ||
| 39 | I've never been late for a date or work | ||
| 40 | I definitely feel useless at times. | ||
| 41 | Sometimes I feel like cursing | ||
| 42 | I almost always feel anxious about something or someone | ||
| 43 | I'm worried about possible failures | ||
| 44 | I'm often afraid that I'm going to blush | ||
| 45 | I often feel overwhelmed by despair | ||
| 46 | I am a nervous and easily excitable person | ||
| 47 | I often notice that my hands shake when I try to do something. | ||
| 48 | I almost always feel hungry | ||
| 49 | I lack self confidence | ||
| 50 | I sweat easily, even on cool days | ||
| 51 | I often dream about things that are better not to tell anyone | ||
| 52 | I very rarely have stomach pain | ||
| 53 | I find it very difficult to concentrate on any task or work | ||
| 54 | I have periods of such intense anxiety that I cannot sit in one place for long | ||
| 55 | I always answer emails immediately after reading them | ||
| 56 | I get upset easily | ||
| 57 | I almost never blush | ||
| 58 | I have much less fears and fears than my friends and acquaintances | ||
| 59 | It happens that I put off until tomorrow what should be done today | ||
| 60 | I usually work under a lot of pressure | ||
Thanks for answers!
Key to the Taylor Personality Anxiety Scale
Description
The Taylor Personality Anxiety Scale is designed to diagnose a subject's anxiety level.
The deceitfulness scale introduced by V.G. Norakidze in 1975, allows us to judge demonstrativeness and insincerity.
The questionnaire consists of 60 statements. For ease of use, each statement is presented to the subject on a separate card.
Key to the test
Anxiety scale:
- Answers “yes” to points are scored 1 point: 6, 7, 9 11, 12, 13, 15, 18, 21, 23, 24, 25, 26, 28, 30, 31, 32, 33, 34, 35, 36, 37, 38, 40, 42, 44, 45, 46, 47, 48, 49, 50, 51, 54, 56, 60;
- “no” answers to items: 1, 3, 4, 5, 8, 14, 17, 19, 22, 39, 43, 52, 57, 58.
Lie scale:
- Answers “yes” to points: 2, 10, 55 are scored 1 point;
- “no” answers to points: 16, 20, 27, 29, 41, 51, 59.
First, you should process the results on the lie scale. It diagnoses the tendency to give socially desirable answers. If this indicator exceeds 6 points, then this indicates the subject’s insincerity.
Then the total score on the anxiety scale is calculated.
Interpretation of the result
40–50 points – considered as an indicator of a very high level of anxiety;
25–40 points – indicates a high level of anxiety;
15–25 points – about the average (with a tendency to high) level;
5–15 points – average (with a tendency to low) level;
0–5 points – low level of anxiety.
Reasons for derealization
The causes of derealization constitute a whole complex: derealization with VSD, derealization with depression, neurasthenia, etc. With prolonged, protracted depression, with the inability to achieve one’s goals, with fatigue, when the psyche can no longer stand it and remains on the sidelines, the body thus turns on protective mechanisms.
At the physiological level of the body, serotonin, norepinephrine, dopamine, GABA noticeably decrease, increased work of the opiate system appears and a person experiences sensations of derealization - this is a lack of pleasure, dulling of feelings, lack of emotions, fear, anxiety, etc. in general, not the reality of the environment.
Treatment
Treatment of derealization is carried out by psychologists, psychotherapists or psychiatrists, who identify the causes of mental disorders and carry out correction and elimination of the symptoms of this pathology. The doctor focuses on treating the underlying disease that led to the development of derealization. For this purpose, different groups of medications are prescribed:
Methods of psychotherapy in combination with autopsychotherapy will be quite effective for finding answers to questions, analyzing one’s own actions, actions, and for drawing conclusions that there is no need to focus on problems.
Methods of art therapy, acupuncture, swimming, massage, and aromatherapy are used.