| Leber's hereditary optic neuropathy | |
| ICD-10 | 47.247.2 |
| ICD-10-CM | H47.22 and H47.2 |
| ICD-9 | 377.16377.16 |
| OMIM | 535000 |
| DiseasesDB | 7340 |
| MeSH | D029242 |
| Media files on Wikimedia Commons | |
Leber hereditary optic neuropathy LHON
, or
Leber optic atrophy
, is an inherited (passed from mother to offspring) mitochondrial degeneration of retinal ganglion cells (GGCs) and their axons, resulting in acute or near-acute loss of central vision; it affects predominantly young men. However, LHON is transmitted only through the maternal line, primarily due to mutations (non-nuclear) in the mitochondrial genome, and only the egg contributes to the mitochondria in the embryo. LHON is typically associated with one of three pathogenic mitochondrial DNA (mtDNA) point mutations. These mutations act on nucleotides and reposition 11778b, 3460b and 14484b, respectively, in the ND4, ND1 and Nd6 subunits of genes in complex I oxidative phosphorylation chains in mitochondria. Men cannot pass the disease on to their offspring.[1]
Causes of the disease, type of inheritance
The disease often progresses in patients aged 12 to 25 years.
, the hereditary factor
plays a significant role in the occurrence of the disease . Clinically, the disease is similar to bilateral retrobulbar neuritis.
During two days
sudden loss of vision develops in both eyes, sometimes the sharpness decreases first in one and then in the other organ.
Over the next two weeks
The quality of vision continues to fall and then stops at a certain level. Complete blindness is relatively rare.
A characteristic feature of Leber's hereditary optic neuropathy is incomplete penetrance
(
up to 40% in men and 15% in women
) and a high incidence of damage among men (they get sick
5 times more often
than women).
This may be due to the effect of an X-linked modifying gene located in the Xp21 region.
The most common causes of the disease are:
- infectious inflammation of the central nervous system and optic nerves;
- congenital and acquired hydrocephalic pathologies;
- cranial oncology;
- cerebral paralysis;
- metabolic disorders;
- intoxication (lead, drugs, mercury);
- congenital and genetic pathologies of the optic nerve.
The following factors influence the development of the disease:
- stress;
- smoking and drinking alcohol;
- exposure to toxins;
- some medications and infections.
Epidemiology
In the Northern European population, approximately one in 9,000 people has one of the three main types of LHON mutations.[11][12] The prevalence of the disease in Europe is between 1:30,000 and 1:50,000.
The LHON ND4 G11778A mutation dominates as the underlying mutation in most countries worldwide, with 70% of cases in Northern Europe and 90% of cases in Asian countries. Due to a founder effect, the LHON T14484C ND6 mutation occurs in 86% of LHON cases in Quebec, Canada.[13]
More than 50 percent of men and more than 85 percent of women with the mutation never experience vision loss or related medical problems. The specific type of mutation can predict the likelihood of penetrance, disease severity, and the likelihood of visual recovery in those affected. Typically, a woman who homoplasmically carries a major LHON mutation has a ~40% risk of having an affected son and a ~10% risk of having an affected daughter.
Additional factors may determine whether a person develops signs and symptoms of this disorder. Environmental factors such as smoking and alcohol consumption may be used, although studies of these factors have yielded conflicting results. Researchers are also studying changes in additional genes, particularly genes on the X chromosome,[14][15] their contribution to the development of signs and symptoms. The degree of heteroplasmy, the percentage of mitochondria that have mutant alleles, may also play a role.[16] Patterns of mitochondrial alleles called haplogroups can also influence the expression of mutations.[17]
Symptoms of Leber's hereditary optic atrophy
In the initial stages of the disease, the fundus of the eye remains unchanged, sometimes only slight hyperemia of the optic nerve papillae
and
blurring of boundaries
.
When diagnosing visual fields, central scotomas are observed.
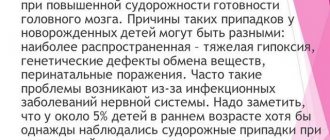
Photo 1. This is what the fundus looks like in the normal state of the organ of vision (on the left) and with atrophy of the optic nerve (on the right).
Atrophy is classified into several types:
- simple (primary) and secondary (post-inflammatory or post-congestive)
- the first is characterized by normal vision loss, narrowing of the lateral visual field; - partial and complete type
- complete or partial loss of vision; - stationary or progressive
- with the first type, the process of vision loss stops at some stage, and with a progressive form, a gradual decline in visual function is observed, which can lead to complete atrophy of the nerve, i.e., blindness; - unilateral and bilateral type
- damage to one or two eyes.
Reference.
Most patients experience progressive deterioration of vision over months or even years, but approximately
20% of patients
experience improvement in vision. There are cases of complete restoration of vision.
The list of symptoms of optic nerve atrophy is quite extensive and depends on the type of pathology. The most common symptoms of all types of pathology:
- decreased visual acuity;
- violation of accommodation;
- night blindness.
In disrepair
disease, in addition to the general symptoms of damage to the visual pathways, signs indicating damage to the central nervous system are added.
This includes cases:
- complicated dementia;
- depression;
- the appearance of bulbar symptoms;
- ataxia of the cerebellar and spinal type;
- spastic paraplegia.
In such situations , differential diagnosis is carried out,
to eliminate the risk of multiple sclerosis, optic nerve or chiasmal tumors.
Attention!
The disease develops at a young age (usually
from 12 to 25 years
), so any signs of visual impairment should not be ignored.
The main symptoms of eye diseases that require contacting an ophthalmologist
- Gradual or sudden deterioration of vision when looking at objects in the distance, the need to strain and squint.
- Sudden, acute pain that weakens when closing the eye is a suspicion of damage to the cornea.
- Constant feeling of a speck in the eye.
- Redness of the eyes, paroxysmal pain, fear of light, whitish or purulent discharge from the eyes.
- Severe headaches accompanied by a decrease in the field of vision.
- There is a veil before the eyes and significant loss of vision.
- Dry eyes.
- Tearing.
- Appearance of “fog” before the eyes.
- Blurry images of objects that were previously seen clearly by others.
Diagnostic methods
Symptoms of optic nerve atrophy appear not only in the early stages of the development of the disease, but also as a result of serious injuries to areas of the brain
, which are responsible for visual functions.
When examining a patient, the doctor examines
the presence of concomitant diseases, facts of taking pharmacology and contact with chemicals, addictions, as well as complaints that indicate possible intracranial lesions.
With physical diagnosis
ophthalmologists determine the presence or absence of exophthalmos, examine the mobility of the eyeball, test the reaction of the pupil to light, and the corneal reflex. Be sure to check visual acuity, perimetry, and study color perception.
List of diagnostic measures:
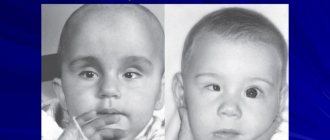
- ophthalmoscopy
- the degree of blurring of the nerve boundary is analyzed;
Photo 2. The ophthalmoscopy process: a special device directs a beam of light onto the eye, which helps to see the patient’s fundus.
- visual acuity test
, determining the boundaries of the visual field; - angiography
of cerebral vessels supplying the nerve; - identification of damaged nerve areas using computer perimetry;
- tomography;
- craniographic examination;
- VEP
, which determines a decrease in lability and an increase in the sensitivity threshold of the optic nerve; - for glaucoma, intraocular pressure is measured;
- plain radiography of the orbit of the eye
- study of pathologies of the orbit; - fluorescein angiography
- examination of the retinal vascular network; - radiography
of the skull and sella turcica; - magnetic resonance imaging (MRI)
- assessment of optic nerve fibers; - blood test
confirming or refuting the presence of an inflammatory process; - ELISA and PCR diagnostics.
Treat eye diseases at ON CLINIC!
In ophthalmology, correct and timely diagnosis is very important. Our clinic is equipped with equipment from the world's best manufacturers, which is distinguished by the highest accuracy of examination results and allows us to identify any pathologies at the earliest stages, when the person himself does not even suspect the existence of vision problems.
The vast experience and professionalism of our ophthalmologists, their focus on advanced international technologies, constant study of new trends in the world of ophthalmology and the successful application of practical developments of foreign colleagues allows us to return the ability to see well to our patients.
Treatment
The disease is dangerous because the destroyed nerve fiber cannot be regenerated.
The effect of therapy can only be due to the restoration of the functioning of fibers that were functional at the time of exposure.
Treatment involves normalizing blood circulation
and
stimulation of vital processes in oppressed nerve fibers
. For this purpose, vasodilating drugs are used, drugs that improve trophic properties and also stimulate the central nervous system.
Important!
Treatment of the disease is more effective when the drug remains in the damaged area for a long time.
To obtain the maximum effect numerous injections are needed
, and this is quite painful.
Irrigation therapy
will allow fractional administration of drugs. Medicines are delivered through a catheter, which is inserted into the retrobulbar space through an opening in the skin in the lower corner of the orbit. The catheter is closed with a sterile stopper and fixed to the skin with adhesive tape.
In young children, the process is performed under inhalation mask anesthesia. For older people - under local. Medicines are administered 5-6 times a day
by piercing the catheter plug with a syringe needle after pre-treatment with ethyl alcohol.
The doctor selects a set of medications depending on the stage of the disease. The treatment period is 7-10 days.
Description:
Leber optic atrophy (Leber optic atrophy) is a hereditary disease characterized by rapidly or gradually developing bilateral central vision impairment in somatically healthy young people.
History of the problem research. The disease was first described by Theodor Leber in 1871, who reported 15 patients from four families. Subsequently, many authors published their observations of families from Europe, Asia, America, Africa and Australia, whose members had been diagnosed with optic neuropathy for several generations.
Causes of Leber's hereditary optic neuropathy:
The attention of most researchers was focused on studying the mechanisms of inheritance of pathology. The intricacy of the problem of studying the mechanisms of inheritance of Leber's optic neuropathy lies in the fact that the disease is transmitted exclusively through the maternal line and develops predominantly in males. In 1963, A. van Senus proved that it is never transmitted by men. At the same time, with X-linked recessive diseases, the expected incidence of female involvement does not exceed 1%, which is significantly lower than the level observed with Leber optic neuropathy. Based on these contradictory facts, DC Wallace (1970) concluded: “A superficial examination of the affected family gives the impression of sex-linked inheritance. The researcher completing the work may assume cytoplasmic inheritance. A more detailed analysis leads to confusion.” In his subsequent works, he emphasized the importance of extrachromosomal maternal factors. Some authors did not exclude the possibility of transfer of persistent virus-like substances into the maternal ovoplasm or transplacental damage to the embryo.
At the same time, the influence of environmental factors on the course of the disease was studied. J. Wilson (1965) found a correlation between the severity of clinical manifestations of Leber's optic neuropathy and smoking. Based on his observations, he suggested that disturbances in cyanide metabolism underlie visual disturbances in patients with Leber optic neuropathy. Later TA. Berninger et al. (1989) found an increase in blood cyanide levels in patients with optic neuropathy in the acute phase. K. Tsao et al. (1999) confirmed the correlation of smoking experience and volume with the penetrance and expressiveness of Leber optic neuropathy.
Genetic research. It has now been proven that the development of Leber neuropathy is caused by point mutations in mitochondrial DNA, leading to the replacement of one amino acid with another. The presumed mitochondrial inheritance of Leber optic neuropathy was confirmed in 1988 by DC Wallace et al., who were the first to identify a mitochondrial DNA mutation point at nucleotide position 11778 in patients with Leber optic neuropathy from nine families. As a result of this mutation, arginine is replaced by histidine in codon 340 of the NADP dehydrogenase subunit 4 gene. Mutation 11778 was identified in 50-60% of all families examined by geneticists whose members had Leber neuropathy.
Another pathogenetically significant (primary) mutation at position 3460 of mitochondrial DNA in patients with Leber neuropathy from three families, in whose members the 11778 mutation was not detected, was established by K. Huoponen et al. (1991). This mutation in column 52 of the gene encoding subunit 1 of NADP dehydrogenase results in the replacement of alanine with threonine. Later N. Howell et al. (1991), as well as DR Johns (1992) identified a mutation at nucleotide position 3460 in another 15 families of patients with Leber optic neuropathy. A mutation at point 3460 has been identified in approximately 8% of patients with Leber neuropathy.
Soon mutations were discovered at nucleotide positions 15257 and 15182 in the apocytochrome b gene. In a study of 120 families whose members had Leber optic neuropathy, mutation 15257 was identified in 8% of pedigrees.
D. Besch et al. (1999) identified a primary point mutation of mitochondrial DNA at nucleotide position 14568 in a patient with Leber's optic neuropathy, his mother and four unaffected members of this family on the maternal side. This mutation caused the replacement of glycine with a series in the ND6 gene. The proband's mother did not have visual disorders, but peripapillary microangiopathy was detected.
This is not the entire list of mutations identified in patients with Leber optic neuropathy. Currently, about 20 point mutations are known. In all cases, they affect the components of the complexes (and the III respiratory chain of oxidative phosphorylation.
Complex 1 (NADH dehydrogenase complex) is the largest protein component of the respiratory chain, containing more than 22 polypeptide chains encoded by both mitochondrial and nuclear genomes. It was found that the G3460A mutation in the ND1 gene in cultured fibroblasts leads to a decrease in NADH dehydrogenase activity by up to 40% compared to normal, while ATP synthesis associated with complex I remains unchanged.
V. Carelli et al. (1999) studied the effect of mutations 14459 and 14484 in the ND6 subunit (Met 64 Val) on complex I. Mutation 14459 was identified in patients with Leber optic neuropathy combined with muscular dystonia. This mutation induces restoration of the specific activity of the NADH dehydrogenase complex and increases its sensitivity to decylubiquinol, a substrate of the L-C| complex. respiratory chain (complex II). Thus, complex I is inhibited by the product of the reaction it catalyzes. Mutation 14484 does not have a similar effect on the specific activity of complex I, but causes a higher sensitivity of this enzyme complex compared to non-mutated forms to inhibitors - ubiquinone analogues.
Analysis of 70 different sequences of the ND6 subunit showed that mutation 14484 affects the most conserved region of the protein molecule, locally reminiscent of the region of cytochrome b that interacts with ubiquinone or ubiquinol in the cytochrome oxidase complex (complex III).
Thus, all mutations affect the oxidative phosphorylation system, thereby disrupting energy metabolism in the cell. According to the hypothesis of A. Sadun (1998), as a result of a decrease in the number of ATP molecules below a certain threshold level, the anterograde axonal transport of mitochondria is blocked, which leads to ATP deficiency and ultimately to the death of the neuron.
Identification of the diagnosis using mitochondrial DNA analysis showed that Leber optic neuropathy covers a wider age range, and women are affected much more often than previously thought. N. Thicme et al. (1999) reported a family in which 9 members had Leber optic neuropathy caused by the ND4 subunit 11778 mutation, eight of them girls under 10 years of age.
Five mutations (11778, 3460, 14484, 15257, and 14568) together account for over 90% of the point mutations identified in all pedigrees with the Leber optic neuropathy phenotype. It is assumed that each of them has a primary pathogenetic significance. Several secondary mutations have also been identified that, acting as synergists in combination, can cause the development of Leber optic neuropathy.
R.I. Oostra et al. (1994) examined the distribution of 7 mitochondrial DNA mutations and their association with clinical manifestations of Leber optic neuropathy in 334 patients from 29 families. Mutations at nucleotide positions 11778, 3460 and 14484, found only in Leber optic neuropathy, were found in 15, 2 and 9 families, respectively. None of these mutations were identified in 3 families. Mutations at nucleotide positions 15257, 13708, 4917, and 4216, which were previously found in both patients with Leber optic neuropathy and healthy controls, were identified in families 1, 10, 3, and 12, respectively. Combinations of mitochondrial DNA mutations were found in members of the majority of families examined. In patients from 11 families in which only one mutation, 11778, was identified, the disease manifested itself at an average age of 29.2 years, and the final visual acuity averaged 0.113. The severity of phenotypic manifestations of Leber optic neuropathy in patients with mutations in other nucleotide positions depended on the mitochondrial genotype.
In families of patients with Leber optic neuropathy, the phenomenon of heteroplasmy has been described: the amount of mutant mitochondrial DNA varies in different patients from 5 to 300% of all available mitochondrial DNA. The disease develops in cases where the percentage of mutant DNA reaches a threshold value. The amount of mutant DNA in the body's cells correlates with the severity of clinical symptoms. During evolution, heteroplasmy of mitochondrial DNA can be effectively maintained over several generations. At the same time, in some individuals, fixation of one of the forms of mitochondrial DNA is possible as a result of the random complete elimination of another form during oogenesis. Thus, in some cases, due to heteroplasmy in the mother, mutant DNA is not passed on to children. M.T. Lott et al. (1990) reported pedigrees in which the amount of mutant DNA increased from generation to generation, correlating with the severity of phenotypic manifestations. The authors also found that the levels of mutant DNA in blood and hair varied within the same subject. Thus, detection and quantification of heteroplasmy is extremely important for diagnosis, prognosis and determination of phenotypic expression.
Although Leber optic atrophy is traditionally considered a family hereditary disease, nowadays clinicians quite often observe patients in whom the manifestation of the disease can be considered sporadic. Familial cases of Leber optic neuropathy accounted for 43% of the total number of patients for the 11778 mutation, 78% for the 3460 mutation, 65% for the 14484 mutation, and 57% for the 15257 mutation.
Notes
- Bandelt HJ, Kong QP, Parson W., Salas A.
More evidence for non-maternal inheritance of mitochondrial DNA? (English) // Journal of Medical Genetics (English) Russian. : journal. — 2005. — December (vol. 42, no. 12). - P. 957-960. - doi:10.1136/jmg.2005.033589. - PMID 15923271. - Leber T. Ueber hereditaere und congenital angelegte sehnervenleiden (1871) Graefes Arch Clin Exp Ophthalmol. 17:249-291
- Erickson RP
Leber's optic atrophy, a possible example of maternal inheritance (English) // American Journal of Human Genetics (English) Russian. : journal. - 1972. - Vol. 24, no. 3. - P. 348-349. - Wallace DC, Singh G., Lott MT, Hodge JA, Schurr TG, Lezza AM, Elsas LJ 2nd, Nikoskelainen EK
Mitochondrial DNA mutation associated with Leber's hereditary optic neuropathy (English) // Science: journal. - 1988. - Vol. 242, no. 4884. - P. 1427-1430. - doi:10.1126/science.3201231. - PMID 3201231. - Huoponen K., Vilkki J., Aula P., Nikoskelainen EK, Savontaus ML
A new mtDNA mutation associated with Leber hereditary optic neuroretinopathy (English) // American Journal of Human Genetics (English)Russian. : journal. - 1991. - Vol. 48, no. 6. - P. 1147-1153. - Johns DR, Neufeld MJ, Park RD
An ND-6 mitochondrial DNA mutation associated with Leber hereditary optic neuropathy // Biochemical and Biophysical Research Communications (English) Russian. : journal. - 1992. - Vol. 187, no. 3. - P. 1551-1557. - doi:10.1016/0006-291x(92)90479-5. - Nikoskelainen EK, Marttila RJ, Huoponen K., et al.
Leber's “plus”: neurological abnormalities in patients with Leber's hereditary optic neuropathy (English) // Journal of Neurology, Neurosurgery and Psychiatry (English) Russian. : journal. - 1995. - August (vol. 59, no. 2). - P. 160-164. - doi:10.1136/jnnp.59.2.160. - PMID 7629530. - cardiac arrythmia
- Mayo Clinic: Multiple Sclerosis
- OMIM 535000
- Man PY, Griffiths PG, Brown DT, Howell N., Turnbull DM, Chinnery PF
The Epidemiology of Leber Hereditary Optic Neuropathy in the North East of England // American Journal of Human Genetics (English) Russian. : journal. - 2003. - February (vol. 72, no. 2). - P. 333-339. - doi:10.1086/346066. - PMID 12518276. - Puomila A., Hamalainen P., Kivioja S., et al.
Epidemiology and penetrance of Leber hereditary optic neuropathy in Finland (English) // European Journal of Human Genetics (English) Russian. : journal. - 2007. - October (vol. 15, no. 10). — P. 1079—1089. - doi:10.1038/sj.ejhg.5201828. - PMID 17406640. - Laberge AM, Jomphe M., Houde L., et al.
A “Fille du Roy” Introduced the T14484C Leber Hereditary Optic Neuropathy Mutation in French Canadians // American Journal of Human Genetics (English) Russian. : journal. - 2005. - Vol. 77, no. 2. - P. 313-317. - doi:10.1086/432491. - PMID 15954041. - Hudson G., Carelli V., Horvath R., Zeviani M., Smeets HJ, Chinnery PF
X-Inactivation patterns in females harboring mtDNA mutations that cause Leber hereditary optic neuropathy (English) // Molecular Vision (English) Russian. : journal. - 2007. - Vol. 13. - P. 2339-2343. - PMID 18199976. - Hudson G., Keers S., Yu Wai Man P., et al.
Identification of an X-Chromosomal Locus and Haplotype Modulating the Phenotype of a Mitochondrial DNA Disorder // American Journal of Human Genetics (English) Russian. : journal. — 2005. — December (vol. 77, no. 6). — P. 1086—1091. - doi:10.1086/498176. - PMID 16380918. - Chinnery PF, Andrews RM, Turnbull DM, Howell NN
Leber hereditary optic neuropathy: Does heteroplasmy influence the inheritance and expression of the G11778A mitochondrial DNA mutation? (English) // American Journal of Medical Genetics (English) Russian. : journal. - 2001. - January (vol. 98, no. 3). - P. 235-243. - doi:10.1002/1096-8628(20010122)98:3<235::AID-AJMG1086>3.0.CO;2-O. - PMID 11169561. - Hudson G., Carelli V., Spruijt L., et al.
Clinical Expression of Leber Hereditary Optic Neuropathy Is Affected by the Mitochondrial DNA-Haplogroup Background // American Journal of Human Genetics (English) Russian. : journal. - 2007. - August (vol. 81, no. 2). - P. 228-233. - doi:10.1086/519394. - PMID 17668373. - Hoegger MJ, Lieven CJ, Levin LA
Differential production of superoxide by neuronal mitochondria // BMC Neurosci: journal. - 2008. - Vol. 9. - P. 4. - doi:10.1186/1471-2202-9-4. - PMID 18182110. - ↑ 1 2 Qi X., Sun L., Hauswirth WW, Lewin AS, Guy J.
Use of mitochondrial antioxidant defenses for rescue of cells with a Leber hereditary optic neuropathy-causing mutation (English) // JAMA: journal. - 2007. - February (vol. 125, no. 2). - P. 268-272. - doi:10.1001/archopht.125.2.268. - PMID 17296905. - ↑ 1 2 Ghelli A., Porcelli AM, Zanna C., Martinuzzi A., Carelli V., Rugolo M.
Protection against oxidant-induced apoptosis by exogenous glutathione in Leber hereditary optic neuropathy cybrids (English) // Investigative Ophthalmology & Visual Science (English)Russian : journal. — 2008. — February (vol. 49, no. 2). — P. 671—676. - doi:10.1167/iovs.07-0880. - PMID 18235013. - GeneTests LHON search (inaccessible link)
- ↑ 1 2 Klopstock, T.;
Yu-Wai-Man, P., Dimitriadis, K., Rouleau, J., Heck, S., Bailie, M., Atawan, A., Chattopadhyay, S., Schubert, M., Garip, A., Kernt , M., Petraki, D., Rummey, C., Leinonen, M., Metz, G., Griffiths, PG, Meier, T., Chinnery, PF A randomized placebo-controlled trial of idebenone in Leber's hereditary optic neuropathy ( English) // Brain (English) Russian. : journal. - Oxford University Press, 2011. - 25 July (vol. 134, no. 9). - P. 2677. - doi:10.1093/brain/awr170. - ↑ 1 2 Shrader WD, Amagata A., Barnes A., Enns GM, Hinman A., Jankowski O., Kheifets V., Komatsuzaki R., Lee E., Mollard P., Murase K., Sadun AA, Thoolen M ., Wesson K., Miller G.
α-Tocotrienol quinone modulates oxidative stress response and the biochemistry of aging. (English) // Bioorganic & medicinal chemistry letters. - 2011. - Vol. 21, no. 12. - P. 3693—3698. - doi:10.1016/j.bmcl.2011.04.085. — PMID 21600768. [] - Sadun A.A., Salomao S.R., Berezovsky A., et al.
SUBCLINICAL CARRIERS AND CONVERSIONS IN LEBER HEREDITARY OPTIC NEUROPATHY: A PROSPECTIVE PSYCHOPHYSICAL STUDY (English) // Trans Am Ophthalmol Soc: journal. - 2006. - Vol. 104. - P. 51-61. - PMID 17471325. - Carelli V., Ross-Cisneros FN, Sadun AA
Mitochondrial dysfunction as a cause of optic neuropathies (English) // Prog Retin Eye Res: journal. — 2004. — January (vol. 23, no. 1). - P. 53-89. - doi:10.1016/j.preteyeres.2003.10.003. - PMID 14766317. - Katz, Jason;
Patel, Chetan. Parkland Manual of Inpatient Medicine (unspecified). - Dallas, TX: FA Davis, 2006. - P. 903. - Clinical Idebenone trial recruiting at Newcastle University UK https://lhon.ncl.ac.uk
- Mashima Y., Kigasawa K., Wakakura M., Oguchi Y.
Do idebenone and vitamin therapy shorten the time to achieve visual recovery in Leber hereditary optic neuropathy? (English) // J Neuroophthalmol : journal. - 2000. - September (vol. 20, no. 3). - P. 166-170. - doi:10.1097/00041327-200020030-00006. - PMID 11001192. - Archived copy (unspecified)
(inaccessible link). Retrieved June 5, 2011. Archived September 4, 2011. Sadun,A et al. "EPI-743 alters the natural history of progression of Leber hereditary optic neuropathy." AOS meeting. May 2011] - Newman NJ, Biousse V., David R., et al.
Prophylaxis for second eye involvement in leber hereditary optic neuropathy: an open-labeled, nonrandomized multicenter trial of topical brimonidine purite // American Journal of Ophthalmology (English) Russian. : journal. - 2005. - September (vol. 140, no. 3). — P. 407—415. - doi:10.1016/j.ajo.2005.03.058. - PMID 16083844. - Haroon MF, Fatima A, Scholer S, et al.
Minocycline, a possible neuroprotective agent in Leber's hereditary optic neuropathy (LHON): Studies of cybrid cells bearing 11778 mutation (English) // Neurobiology of Disease (English)russian. : journal. - 2007. - Vol. 28, no. 3. - P. 237-250. - doi:10.1016/j.nbd.2007.07.021. - PMID 17822909. - Clinical Curcurmin trial recruiting at ClinicalTrials.nlm.nih.gov Archived February 13, 2009.
- Wisconsin near infrared trial Archived May 15, 2008.
- Craven L., Tuppen HA, Greggains GD, Harbottle SJ, Murphy JL, Cree LM, Murdoch AP, Chinnery PF, Taylor RW, Lightowlers RN, Herbert M., Turnbull DM
Pronuclear transfer in human embryos to prevent transmission of mitochondrial DNA disease ( English) // Nature: journal. - 2010. - May (vol. 465, no. 7294). - P. 82-85. - doi:10.1038/nature08958. - PMID 20393463.
Symptoms of Leber's hereditary optic neuropathy:
Clinically, there is an acute onset of vision loss, first in one eye, and then after a period of several weeks to several months in the other. Onset usually occurs in adolescence, but there have been reports of onset ages ranging from 7 to 75 years. The starting age is slightly higher for women (range 19–55 years: mean 31.3 years) than men (range 15–53 years: mean 24.3 years). The ratio between males and females varies depending on the mutations: 3:1 for 3460 G>A, 6:1 for 11,778 G>A and 8:1 for 14484 T>C.
This usually develops into very severe optic atrophy and permanent loss of visual acuity, affecting both eyes simultaneously (25% of cases) or sequentially (75% of cases) with an average interval of 8 weeks. Only in rare cases can only one eye be affected. In the acute stage, lasting several weeks, the affected eye exhibits the appearance of swelling of the nerve fiber layer, especially in the arcuate fasciculi and enlarged or telangiectatic and tortuous peripapillary vessels (microangiopathy). The main features are visible under ophthalmoscopy, before or after loss of vision. Pupil defects may also be visible in the acute stage. Analysis shows decreased visual acuity, loss of color vision, and typhlocentral scotoma on visual field testing.
“LHON Plus” is the name given to rare cases of eye disease in the presence of other conditions. Symptoms of this higher form of the disease include loss of the brain's ability to control muscle movement, and cardiac arrhythmia. In many cases, LHON Plus has been comparable to multiple sclerosis due to the lack of muscle control.
Treatment of Leber's hereditary optic neuropathy:
Without knowledge of the family history of LHON, diagnosis typically requires a neuro-ophthalmologic evaluation and blood testing for mitochondrial DNA assessment. It is important to rule out the influence of other possible causes of vision loss and important, associated syndromes such as cardiac electrical conduction system abnormalities. The prognosis for victims who remain incurable is almost always continued to be significant in both eyes. Regular visual acuity tests and perimetry checks are recommended for next steps for affected individuals. There is excellent therapy for some cases of this disease, especially those with early onset. In addition, experimental treatment protocols are ongoing. Genetic counseling should be offered. Health and lifestyle must be reconsidered, especially in light of toxic and nutritional theories of gene expression. Sighted assistants and rehabilitation services should be used to help maintain jobs.
For those who carry the LHON mutation, preclinical markers can be used to monitor progress. For example, fundus photography can monitor swelling of the nerve fiber layer. Optical coherence tomography can be used to study the thickness of the retinal nerve fiber layer in more detail. Red-green color perception testing can detect loss. Contrast sensitivity may be reduced. An abnormal electroretinogram or visual evoked potential may be detected. Neuron enolase and blood neurofilament heavy chain axonal markers can predict conversion status for those affected.
Cyanocobalamin (a form of vitamin B12) should be avoided as it can cause blindness in patients with Leber's disease.
It is generally recommended to avoid optic nerve toxins, especially tobacco and alcohol. Some prescription drugs are known to carry potential risks, so all drugs should be treated with suspicion and the risk assessed before use. Ethambutol, in particular, has been implicated as a trigger for vision loss in LHON carriers. Indeed, toxic and nutritional optic neuropathies may have overlapping symptoms, mitochondrial mechanisms of disease and management with LHON. It should be noted that when a patient as a result of LHON or toxic/nutritional optic neuropathy has suffered a complicating disease process, nitroprusside (trade name: Nipride) should not be used due to the increased risk of optic ischemia as a consequence of the reaction to this antihypertensive drug.
Idebenone, in a small placebo-controlled study, was shown to achieve moderate benefit in approximately half of patients. The best results were in people who were at the onset of the disease.
α-Tocotrienol-quinone, a metabolite of vitamin E, has had some success in reversing incipient vision loss in small open-label studies.
There are various treatment approaches that have been in preliminary trials or proposals, none have yet provided convincing evidence of usefulness and safety for treatment or prevention, including: brimonidine, minocycline, curcumin, glutathione, infrared phototherapy, and viral vector techniques.
"In Vitro Fertilization in a Third Party" is a proof of concept research methods for preventing mitochondrial disease in human fetal development. So far, viable macaques have been produced. But ethical and educational obstacles have stopped the method from being used in humans.
A mitochondrial neurodegenerative disease affecting the optic nerve, often characterized by sudden loss of vision.
Prevalence
This disease is not known exactly, but is estimated at 2-4 cases per 100,000 population.
NOPD occurs as a result of a mutation in mitochondrial DNA (mtDNA). It has been proven that stress, smoking, alcohol, toxins, viruses, and taking certain medications can serve as trigger mechanisms for the disease.
Clinic.
The disease manifests itself as a sudden, painless, acute/subacute loss of central vision, usually between the ages of 18 and 30 years.
With NOPD, either both eyes are affected simultaneously or sequentially with an interval of several weeks or months after the first. More often, vision loss occurs subacutely over several weeks, then the condition stabilizes. However, in many patients, the size of the central scotoma continues to expand for several years, leading to profound blindness.
In the early stages of vision damage, disturbances in red and green color perception and contrast may be observed.
Other neurological symptoms may also be present. These disorders are known as Leber plus and include movement disorders, dystonia, postural tremors, and cerebellar ataxia.
Diagnosis
placed on the basis of ophthalmoscopic examination. Fundamental findings of NPHL include papilledema, tortuous vessels, peripapillary telangiectasias, microangiopathy, and central scotomas on visual field testing.
Optical coherence tomography (OCT) helps confirm swelling of the retinal nerve fiber layer. Even before vision loss occurs in patients who carry the mutation, it is possible to detect a disturbance in red-green color perception, as well as reduced or borderline electroretinogram and visual evoked potentials.
In differential diagnosis, first of all, multiple sclerosis should be excluded, in which optic neuritis is a common symptom. It is also necessary to exclude other genetic optic neuropathies, such as Wolfram syndrome and classic autosomal dominant types of optic atrophy.
Treatment.
There is no specific treatment for NOPD. The main supportive therapy is drugs for the visually impaired. Several substances have shown positive results in restoring vision. A synthetic analogue of coenzyme Q10, idebenone, improved vision after a year of use.
A third generation of quinones is currently being tested and there are also reports of beneficial effects. It is very important that the patient avoid the use of alcohol, tobacco and certain antibiotics, which also affect mitochondrial oxidative phosphorylation.
Forecast
The disease depends on the age of onset of symptoms. Young people have a more favorable prognosis. With some mutations, spontaneous partial restoration of vision has been described 1-2 years after the onset of the disease. In 30-50% of men and 80-90% of women who carry the mutation, blindness does not occur. Complete blindness develops extremely rarely.
Link to Orphanet
| Leber optic atrophy |
Reference
Today in Russia, diseases with a prevalence of no more than 10 cases per 100,000 people are considered rare.
215 diseases are included in the list of orphan diseases in Russia. (list from the Ministry of Health dated May 7, 2014)
We would also like to draw your attention to the following documents that we have added to the relevant sections of our Encyclopedia.
Leber Hereditary Optic Neuropathy (NOHL or LHON), also known as Leber Optic Atrophy (LOA), is named after Dr. Theodore Leber, who described it in 1871 as a characteristic pattern of sudden loss of vision in young people with a family history of loss of vision was observed. It is the most common hereditary optic neuropathy and is caused by a mitochondrial mutation and its prevalence is very low and unknown in most geographic areas. In the north-east of England and Finland, the disease affects 1 in every 31,000 or 50,000 people respectively.
It is usually seen in young men aged 18 to 35, although it can also affect younger children and adults over 35. In women it is much less common.
It usually causes severe vision loss in both eyes. In most cases, the process begins in one eye and moves to the other eye after a few weeks or months.
Why is it produced? What is mitochondrial heredity?
Although the vast majority of our genetic material (DNA) is located in the nucleus of our cells, a small portion is found in the mitochondria (mitochondrial DNA or mtDNA).
Core genes are inherited from both biological parents. However, mitochondrial DNA is inherited only from the mother. This means that a man with a mutation in mitochondrial DNA will not pass it on to any of his biological descendants, whereas a woman with a mutation in mitochondrial DNA will pass it on to all of her biological descendants.
90-95% of LHON cases are associated with one of three specific mtDNA mutations. However, a significant proportion of people with these mutations never develop symptoms of the disease. Specifically, only 10% of women and 50% of men carrying any of these mutations have optic neuropathy. This implies that other factors, genetic (mitochondrial or nuclear) and/or environmental factors must act so that vision loss occurs. For example, exposure to tobacco or large amounts of alcohol in people carrying these mutations increases the risk of developing the disease.
Symptoms of Leber Optic Neuropathy
Typically, LHON carriers do not have vision until they lose vision significantly quickly in one eye and, after a few weeks or months, in the other eye as well. Vision continues to deteriorate over several weeks until it becomes significant, and in most cases central vision (needed for reading, driving, and recognizing faces) is severely affected in both eyes, although some people experience some vision recovery after some time. This permanent vision loss results from the death of the optic nerve cells responsible for transmitting images from the eyes to the brain.
Although vision loss is the only symptom in most patients with LHON, abnormal heart rhythms as well as neurological changes (such as postural tremors or other movement disorders) have been described in some cases.
How is it diagnosed? Is there a treatment for this disease?
This disease is difficult to diagnose for several reasons. First, it is a hereditary disease, but it does not affect all people who have the mutation. For this reason, it may appear without taking into account a family history of the disease.
To diagnose it, it usually requires a thorough neurophthalmologic evaluation and blood testing to examine mtDNA.
Fundus examination initially shows microangiopathy and swelling of the peripapillary nerve fiber layer, which progresses to optic atrophy.
The current prognosis is usually permanent, severe vision loss. Several treatments for the disease are being explored, and research into the disease is underway at the ICR and is in the screening phase.
Leber's amaurosis is a genetic ophthalmological disease that leads to a significant deterioration in visual function (up to its complete loss). It is based on irreversible damage to the light-sensitive cells of the retina of the eyeball (cones and rods).
Leber's amaurosis is a rare hereditary pathology: it occurs with a frequency of 3 cases for every 100,000 newborns. Approximately every 5th case of congenital blindness or low vision is caused by Leber's amaurosis.
Causes and risk factors
Leber congenital amaurosis is a whole group of retinal dystrophies caused by various genetic causes. Most often, it is inherited in an autosomal recessive manner, that is, for the pathology to develop, the child must receive a mutated gene from both the mother and the father.
The prognosis for Leber amaurosis is negative: children are either irreversibly blind from birth or lose vision during the first ten years of life.
There are several forms of Leber amaurosis, which are inherited in an autosomal dominant manner. In this situation, only one altered gene is sufficient for the occurrence of a dystrophic process in the retina of the eyeball.
Signs and symptoms

Decreased visual response at birth is the first sign of the disease. Often the child pokes, presses and rubs the eyes to stimulate the retina to receive light. This activity can cause the eyes to become sunken or deep-set (enophthalmos).
Other symptoms may include:
- strabismus;
- nystagmus;
- photophobia;
- cataract;
- keratoconus.
In addition, some children may have hearing loss, mental retardation and/or developmental delays.
Forms of the disease
Depending on which gene the mutation occurred in, several types of the disease are distinguished:
- Mutations in the CRX gene, which is responsible for the development of photoreceptors in the embryo, as well as maintaining the required number of them throughout life. Mutations in it cause late pigmentary retinal degeneration, Leber amaurosis type VII and rod-cone dystrophy. All these forms of the disease have an autosomal dominant mode of inheritance.
- Mutations in the LCA5 gene, which encodes the synthesis of the lebercillin protein by retinal cells. Its mutations lead to Leber amaurosis type V with an autosomal dominant mode of inheritance.
- Mutations in the RPE gene It carries the code for the synthesis of a protein specific to the retinal pigment epithelium and plays a leading role in the metabolism of retinol. More than 80 variants of the RPE65 gene mutation have been described, which lead to retinal pigmentary degeneration and Leber amaurosis type II.
- Mutations in the LRAT gene, responsible for the synthesis of microsomal protein - lecithin-retinol acyltransferase (LRAT). It is involved in the process of retinol (vitamin A) metabolism in the cells of the vision system and liver. Gene mutations cause juvenile pigmentary retinal degeneration, Leber amaurosis type XIV.
- Mutations in the CRB1 gene, which encodes the synthesis of a protein necessary for the normal development and functioning of photoreceptors. Currently, over 140 different mutations of this gene are known, which lead to retinal pigmentary degeneration type XII, Leber amaurosis type VIII.
Approximately every 5th case of congenital blindness or low vision is caused by Leber's amaurosis.
Genetics
Leber's hereditary optic neuropathy has a mitochondrial pattern of inheritance.
Leber's hereditary optic neuropathy is a condition associated with changes in mitochondrial DNA. Although most DNA is packaged in chromosomes within the nucleus, mitochondria have a distinct mitochondrial genome made up of mtDNA.
Mutations in the MT-ND1, MT-ND4, MT-ND4L and MT-Nd6 genes cause Leber hereditary optic neuropathy.[10] These genes encode the membrane portion of the NADH dehydrogenase protein involved in normal mitochondrial oxidative phosphorylation function. Oxidative phosphorylation uses a series of four large multienzyme complexes, all embedded in the inner mitochondrial membrane, to convert oxygen and monosaccharides into energy. Mutations in any of the genes disrupt this process, causing different syndromes depending on the type of mutation and other factors. It remains unclear how these genetic changes lead to cell death in the optic nerve and other specific symptoms of Leber hereditary optic neuropathy.
Diagnostics
Diagnosis of Leber amaurosis begins with an ophthalmological examination. Then the following methods are used:
- visual evoked potentials (VEPs);
- electroretinography;
- electrooculography.
Electroretinography (ERG) has the greatest diagnostic value. The method allows you to record the bioelectrical activity of retinal neurons. In Leber amaurosis, the ERG is not recorded. In congenital blindness caused by other causes (syphilis, rubella, optic atrophy), the ERG shows a normal or subnormal picture.