10.01.2019
Plexopathies can be cervical, shoulder and lumbosacral, but the most common is the shoulder variant.
Damage to the brachial plexus that occurs in newborns during obstetric procedures is called Duchenne-Erb palsy. The pathology is characterized by a violation of the ability to make rotational movements of the shoulder, move it to the side and lift it. The function of bending the arm at the elbow joint becomes difficult, while the fingers retain relative mobility.
In 1872, Guillaume Duchenne, in his writings, described the pathology of the shoulder region in newborns and suggested that the cause of paralysis was manipulation during obstetrics. Two years later, neuropathologist Wilhelm Erb proved the connection between paralysis and trauma received during obstetrics.
On average, there are 1-2 cases of plexopathy per thousand newborns, so the pathology is considered common. Obstetricians-gynecologists, neurologists, traumatologists, pediatricians and neonatologists, and orthopedists deal with the issues of its treatment and prevention.
The disease can interfere with the full development of the child, worsens the patient’s quality of life, and in adulthood limits the ability to work and leads to disability.
Causes of plexopathy
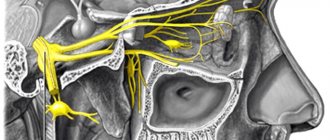
Disorders in the brachial plexus occur as a result of traumatic mechanical effects on its upper trunk, which is formed by the 5th and 6th cervical spinal roots. In adults, plexopathy is relatively rare. It can be caused by trunk injuries due to:
- shocks and falls;
- sudden stretching of the arm;
- deep penetrating wounds.
Particularly common are obstetric paralysis that occurs due to damage to the brachial plexus in infants during childbirth. Nerve tissue ruptures occur as a result of severe stretching of the plexus. Erb's plexopathy occurs after obstetric manipulations:
- turning the child by one of his legs;
- shoulder release;
- extraction by hand;
- extraction by the pelvic end.
Such manipulations are necessary in cases where the fetus is in a breech position, during prolonged labor, weak contractions and pushing. According to statistics, damage to the nerve ganglion of newborns is observed with large fetuses or a narrow pelvis in a woman in labor.
Some children develop torticollis along with plexopathy due to rupture of the cleidomastoid muscle or accessory nerve. Performing obstetrics can lead to a complete rupture of the upper trunk, or a section of it, to injuries to the muscles and fascia, and hemorrhages.
Inflammation and swelling develop in the damaged area, which disappear after a certain time. Subsequent tissue fibrosis (scarring) compresses nerve fibers and blood vessels, causing dysfunction of the area.
Plexopathy: symptoms of the disease
Symptoms include three successive stages.
Acute post-traumatic period. It occurs immediately at the time of injury and lasts up to one month. First, inflammation and swelling develop, and hematomas appear. After a few days, the signs of acute inflammation disappear. The hand does not move away from the body and does not bend at the elbow joint, the palm faces down and the thumb points inward. The movement of the fingers is preserved; in case of paresis, the movements of the arm and shoulder are limited.
The affected limb does not respond to the biceps reflex. The child does not hold the arm horizontally, so it hangs down, and the threshold of pain sensitivity on the lateral surface decreases. In infants, gag and grasping reflexes are weakened.
On the side of the injured area, muscle tone is reduced, local hypothermia and pallor of the skin are observed. The newborn reacts weaker to irritation of skin receptors on the affected area than to the same actions on other parts of the body.

Recovery stage. At the end of the acute period, the recovery stage begins. How much limb function is restored depends on the extent of the damage and subsequent therapy. Mild paresis implies gradual tissue regeneration and gradual restoration of the functions of the upper limb girdle. Range of motion and sensitivity can be fully restored, however, at the age of 3-4 years, the baby experiences decreased muscle tone and shortening of the limb of a relatively healthy arm.
Residual phase. Residual pathological phenomena depend on the success of the recovery stage and the completeness of restoration of tissue innervation. In mild cases, residual effects are mild, manifested mainly by relative shortening of the affected arm and muscle weakness.
With moderate to severe paralysis, the fold of skin at the junction of the shoulder and chest lengthens and becomes deeper, creating a “doll’s hand” effect. Pronation of the shoulder leads to pathological changes in soft tissues and the inability to perform rotational movements. The mobility of the elbow joint is impaired, its extension and the extension of the hand are difficult. Atrophied soft tissues are not able to fully support the shoulder joint, which leads to its dislocations and subluxations even under minor loads. With age, asymmetry of the upper limb girdle develops, leading to scoliosis in the cervical and thoracic region.
Types of obstetric paresis
By severity
obstetric paresis is:
- average
- lungs
- heavy (total).
Obstetric paresis, depending on the location of the damage, is divided into:
— Upper
: In the upper type, which is more common than the lower type, the arm hangs passively, there is no movement in it or can only be preserved in the hand, the arm is usually brought to the body and rotated inward, and the hand is in a position of palmar flexion. The fold between the torso and shoulder is deepened. If the child is lifted, the arm hangs back. Muscle tone is sluggish, passive movements in the joints are preserved.
— Lower
: With lower paralysis, there is no movement of the hand and fingers, the arm hangs down and the child carries it, supporting it with a healthy arm. Atrophy of the small muscles of the hand occurs, as a result of which the proximal phalanges assume a hyperextension position, and the distal ones are bent.
— Total
: Total arm paresis (total type of obstetric arm paresis) occurs as a result of damage to the upper and lower primary bundles of the brachial plexus of the spinal cord or avulsion of nerve roots from the spinal cord.
Diagnosis of Erb-Duchenne plexopathy
Plexitis in newborns is diagnosed based on clinical signs and a history of birth trauma. In adults, the disease must be differentiated from Klumpke's palsy, which primarily affects the hands. The patient is examined by an orthopedist, after which a neurological examination is prescribed. In maternity hospitals, plexitis is diagnosed by a neonatologist.
An X-ray examination is performed to identify abnormalities in the skeletal bones. There is a change in the distance between the scapular articular cavity and the metaphysis of the humerus, atrophic phenomena and osteoporosis.
The diagnosis is confirmed using ultrasound examination of the shoulder joint and magnetic resonance imaging. Assessment of damage to uneven muscle structures is carried out using electromyography, and the functionality of the nerve trunk is carried out using electroneurography.
Prevention
Preventive measures for obstetric paralysis should be aimed primarily at familiarizing those involved in obstetrics (midwives) with complications during childbirth in the form of fractures, dislocations and paralysis that occur as a result of the use of excessive physical force and improper techniques during obstetrics.
Further preventive measures come down to early detection of obstetric paralysis and early treatment. For this purpose, it is necessary to train the staff of maternity hospitals and maternity wards of hospitals (pediatricians, obstetricians) in the early diagnosis of injuries, in particular paralysis.
Children suffering from obstetric paralysis should be registered for further clinical observation and treatment.
The information presented in this article is intended for informational purposes only and cannot replace professional advice and qualified medical care. If you have the slightest suspicion that your child has this disease, be sure to consult a doctor!
Plexopathy: treatment
The sooner complex therapy for pathology in newborns is started, the less pronounced its consequences will be in adult life. Conservative treatment involves immobilizing the injured limb with a splint. It must be worn constantly and removed during therapeutic and hygienic procedures.

Medications are used to eliminate inflammation and reduce pain (nurofen, panadol), improve blood circulation (aminophylline, papaverine), resolve hematomas and edema (hyaluronidase, aloe vera extract), eliminate movement disorders (neostigmine). In addition, injections of group B drugs are prescribed as a stimulator of metabolic processes in neurons.
If pharmacotherapy does not produce the expected effect during the first three months of the baby’s life, the issue of surgical intervention is decided. Neurosurgical operations are performed in cases of complete rupture of the superior column, separation of the spinal roots, and in the absence of flexion function of the elbow joint in children older than three months.
An operation aimed at restoring the integrity of the nerve column is carried out by a neurosurgeon using microsurgery techniques. Surgical treatment is advisable for children under 11-12 months of age, with the best age for surgery being 3-7 months. During this period, the nervous system is not yet fully formed, so regeneration processes are more active.
In addition to pharmacotherapy and surgical treatment, physiotherapy plays an important role in restoring functions, but it should not be used in the acute phase of the disease. Physiotherapeutic interventions are carried out in courses after pain relief. On average, the course of treatment is 10-15 sessions.
Reflexology, including acupuncture, provides results. Several times a year, the baby needs to undergo an outpatient course of electrophoresis and electrical stimulation. Balneotherapy, paraffin, wax or mud applications are recommended for treatment.
Signs of obstetric paresis
With obstetric paresis, there is a significant decrease in muscle tone (muscle hypotonia). As a rule, the affected limb hangs along the body, all joints are straightened. Muscle hypotonia in the paretic arm is pronounced. Active movements are completely absent, only slight movements in a supine position are possible. The skin of the hand affected by paresis is pale and cold to the touch. Early development of muscle atrophy, especially in the distal regions. Reduced pain threshold and temperature sensitivity throughout the entire limb. There are no tendon reflexes. The hand lacks grasping and palmo-oral reflexes.
The degree of muscle damage varies: from a slight decrease in muscle strength and tone to deep functional disorders, characterized by a complete absence of active movements. Identification of the localization and depth of motor disorders is necessary for correctly informed implementation of therapeutic measures.
What to do if your child has obstetric paresis?
If obstetric paresis is detected in a child, you must immediately contact a specialist. At the first stage, the doctor prescribes an examination of the damaged limbs to determine the degree of damage to the nerve roots. Based on the examination results, the doctor prescribes a course of treatment: conservative or surgical.
Consultations and surgical treatment are carried out by reconstructive microsurgeon Mikhail Leonidovich Novikov.
You can get preliminary organizational consultation and ask questions by calling 8-800-555-84-21 or leaving a message in the on-line consultation form in the right column of the site.
Surgical treatment is provided free of charge with the support of Rusfond. In order for treatment to be free, you need to collect documents, send them for verification and registration (can be scanned in color by email: website), then wait for a call for treatment.
Treatment of plexopathy with traditional methods
Traditional medicine is not able to effectively combat plexopathy, however, some remedies can be used as a complement to conservative therapy.
- Cabbage compress. Soften the cabbage leaf over steam and apply it to the shoulder joint, put gauze on top, folded in several layers, secure with a bandage and leave for 4-8 hours.
- Rubbing with ammonia. Beat a chicken egg with a whisk, add 10 ml of ammonia and 10 ml of turpentine. Rub the affected area before going to bed.
- Bath with mint. Boil 5-7 tablespoons of mint leaves for 2-3 minutes and leave. Pour the decoction into a bath with warm water and take for 15-20 minutes.
- Ointment with propolis. Melt 15 g of animal fat in a water bath, add 1 gram of propolis, mix thoroughly and let the mixture cool. Rub into the shoulder with massage movements 2-3 times a day.
- Ointment with medicinal herbs. Grind 5 grams of dried sweet clover, St. John's wort and hop cones in a mortar to a powder and mix thoroughly with 25 grams of Vaseline. Rub into the shoulder joint area overnight.
Disease prognosis
The disease does not pose a threat to the patient's life. At the same time, dysfunction of the hand leads to delays in the physical development of the child, deformations of the spinal column, decreased ability to work in adults and the quality of life in general.
Timely treatment for incomplete ruptures of nerve fibers allows you to completely avoid the consequences of birth trauma. In such patients, the prognosis is favorable, since over time the function of the shoulder and elbow joint is restored, and the person lives a full life.
With complete avulsions of the spinal roots, the patient partially loses sensitivity, muscle tone in this area is reduced. Lack of treatment leads to muscle atrophy and soft tissue degeneration.