Main symptoms:
- Rapid overgrowth of fontanel
- Convex forehead
- Headache
- Deformation of the facial structure
- Skull deformation
- Moodiness
- Sleep disturbance
- Underweight in newborns
- Insufficient development of the lower jaw
- Mental retardation
- Retarded physical development
- Absence of some reflexes
- Mood swings
- Tearfulness
- Poor appetite
- Vomit
- Nausea
- Enlargement of the occipital protuberance
- Enlarged eye sockets
- Frequent regurgitation
Scaphocephaly (sagittal craniostenosis) is a pathology of the formation of the shape of the skull, in which there is premature healing of one or more sutures of the skull. The main pathological process is craniostenosis, scaphocephaly is only its most common subtype.
Online consultation on the disease “Scaphocephaly”.
Ask a question to the specialists for free: Neurologist.
- Etiology
- Classification
- Symptoms
- Diagnostics
- Treatment
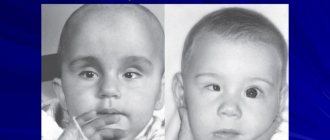
The pathology is clearly visible already in infancy: the skull is elongated and irregular in shape, there is depression of the temples and overhang of the frontal zone.
This is not just about a cosmetic defect. Head circumference parameters exceed age norms, the brain does not fully develop, which leads to the development of associated complications. A syndrome such as scaphocephaly can have a negative impact on development, but only if treatment is not started in a timely manner.
The exact cause of the development of pathology in a child has not yet been established; clinicians identify only a number of predisposing factors.
Treatment is surgical. If the child is under six months old, endoscopy is used as an analogue and as a more gentle method, which allows, although not eliminating, but minimizing the development of complications.
The pathology does not pose a threat to the child’s life and does not negatively affect development, but only if therapy is started in a timely manner. This syndrome in adults clearly leads to persistent mental and psychological disorders.
Skull sutures
Treatment of the disease
Treatment for craniosynostosis involves surgery in a specialized clinic. Today, the techniques are so well developed that patients almost never experience complications. The earlier craniosynostosis is diagnosed in a child, the greater the chances of a successful outcome of the operation, the better the cosmetic result (appearance of the face and skull).
The brain grows most actively when the child is not yet 2 years old. By the time a child reaches his 2nd birthday, his brain already has 90% of the volume of an adult. Therefore, craniostenosis can be prevented only through early surgical intervention. Doctors believe that the disease in question can be effectively treated at the age of 6-9 months. Because the bones of the infant's skull are easy to manipulate at this age, the final remodeling of the skull's shape by the rapidly growing brain is facilitated. At the age of 6-9 months, the child's residual bone defects heal more fully and quickly.
If the disease is diagnosed late and the child undergoes surgery when he is already 3 years old, then there is almost no chance that the functions of the eyes and brain will improve. The operation in such cases will only improve the appearance of the child, nothing more. Modern treatment allows not only to increase cranial volume, but to correct its shape to a more or less correct one.
Treatment is most effective with the collaboration of an oral and maxillofacial surgeon and a neurosurgeon.
Surgical treatment:
- remodeling of the bones of the cranial vault. To do this, the bones of the deformed areas are removed and rearranged into the correct anatomical position, as a result of which the cranial cavity is enlarged;
- dissection of fused sutures in early childhood (when persistent deformation of the skull has not yet developed);
- reconstructive surgery for developed skull deformation (elimination of skull defects, correction of its shape).
To date, new, less traumatic methods have been developed using endoscopic techniques to minimize blood loss, reduce the severity of swelling, pain and reduce the patient’s time in the hospital. However, this approach is only possible for children under six months of age. If the child is older, the treatment will be more intense. Cosmetic problems often require the involvement of a dentist.
What provokes / Causes of Craniosynostosis:
The nature of this disease has been little studied to date. But there are a large number of theories about the occurrence of craniostenosis. Theories suggest the following reasons:
- hormonal
- intrauterine
- hereditary disorders
- compression of the fetal head in the uterus, etc.
One of the pathogenesis factors is officially recognized by medicine as a defect in the fibroblast growth factor receptor gene (FGFR) 1,2,3.
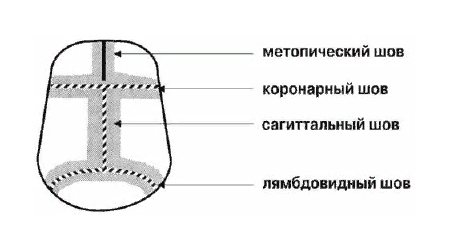
The main sutures of the cranial vault:
- coronary
- sagittal
- metopic
- lambdoid
If the bone suture is affected, compensatory bone growth is recorded perpendicular to its axis, which is called Virchow’s law in the medical literature. As a result of this process, a characteristic deformation occurs - unique for each of the closed seams. Sagittal craniostenosis causes scaphocephaly, and synostosis of the entire coronal suture causes plagiocephaly. If there is synostosis of the metopic suture, trigonocephaly occurs.
Synostosis of the entire lambdoid suture or half of it leads to deformation of the occipital region. Its degree directly depends not only on the degree of synostosis and the number of sutures included in the deformity, but also on the state of the brain itself. For example, if there is hydrocephalus at the same time, then the severity increases.
Diagnosis of the disease
In most cases, a visual examination of the child by a doctor is sufficient to diagnose this type of cranial pathology. However, if for some reason the deformation is not detected visually, they resort to radiographic studies, computed tomography and magnetic resonance imaging.
- Analysis of complaints and medical history: how long ago signs of skull deformation began to appear; whether there were cases of a similar disease in anyone in the family.
- Analysis of the obstetric and gynecological history of the child’s mother: how the pregnancy with this child proceeded; were there any complications during pregnancy (increased arterial (blood) pressure, vomiting, etc.); were there any infectious diseases during pregnancy; whether there was any alcohol consumption during this pregnancy; features of childbirth (for example, injuries to the child during the passage of the birth canal).
- Neurological examination: search for signs of neurological pathology (strabismus, limitation of eye movement in any direction, nystagmus (pendulum-like oscillations of the eyeballs)). In addition, in a newborn it is necessary to palpate (feel) the fontanelles of the skull, because If the seams become fused, they become compacted.
- Craniometry: measuring the size of the skull using a measuring tape.
- Examination of the fundus: signs of increased intracranial pressure may be detected (the sutures are fused, so the volume of the skull does not increase, while the volume of the brain grows. Because of this, intracranial pressure also increases).
- Ultrasound venography of the main veins of the head and neck: allows you to identify signs of impaired outflow of venous blood from the cranial cavity, which indirectly indicates an increase in intracranial pressure.
- Ultrasound examination of the heart: allows you to identify abnormalities in the development of the heart (sometimes found as an anomaly combined with craniostenosis).
- Ultrasound examination of the fetus: allows one to suspect the presence of craniostenosis in a child in utero (by changes in the shape of the head).
The use of modern diagnostic equipment is especially appropriate for the early diagnosis of craniostenosis. The possibility of an adequate diagnosis is hampered by some conditions characteristic of the postnatal period of child development, similar to craniosynostosis, but not pathological. So-called plagiocephaly (positional displacements) can be easily corrected if the child is provided with a certain head position during sleep; much less often when using a special cranial bandage. Craniosynostosis itself, regardless of its clinical picture, requires surgical intervention.
Symptoms of Craniosynostosis:
Sagittal craniosynostosis
With this type of disease, the anteroposterior size of the skull increases, while the width decreases. you can notice that the child’s head is sharply elongated in the longitudinal direction, and the occipital and frontal regions overhang, while the temples seem to be depressed. Such changes lead to the fact that the child’s face becomes oval and narrow. This type of deformation is called scaphocephaly or scaphoid skull.
Nontopic craniosynostosis (trigonocephaly)
Among isolated craniosynostoses, this type is the least common. A triangular deformation of the frontal part of the head is formed, a bone keel is formed, which runs from the glabella to the large fontanel. Hypotellorism is observed. Most doctors consider trigonocephaly as a component of such syndromes as Oro-facio-digital or Opitz. As the child grows, the deformation of the forehead becomes less noticeable due to the fact that the peaks of the ridge are smoothed out and the frontal sinuses develop. But the curvature of the frontal bone is still visible, there is an outward turn of the supraorbital edges, and hypotellorism remains. There may be brain damage, but it cannot be predicted. Visual impairment is likely, and there is a delay in the development of the child’s intelligence.
Unilateral coronary craniosynostosis
In the pathology under consideration, the coronal suture is located perpendicular to the median axis; it consists of two equal halves. If one of them grows prematurely, a typical asymmetric deformation occurs, which in the medical literature is called plagiocephaly. In the child, the superior orbital edge of the orbit and frontal bone on the side that is affected becomes flattened. And the other half of the forehead droops - a compensatory mechanism of development.
The older the child becomes, the more flattening of the zygomatic region becomes apparent, and the nose becomes bent in the unaffected direction. From about 6-7 years of age, the bite begins to deform because the height of the upper jaw becomes larger. The consequence of this is a displacement of the lower jaw on the side of the prematurely closed suture.
Vision is impaired with this type of craniosynostosis, most often strabismus. Plagiocephaly can be mistaken for features of the postnatal head configuration, but it does not disappear in the first 14-21 days of life.
Bilateral coronary craniosynostosis
It occurs in approximately 15-20 cases out of 100. In such cases, a wide, flattened forehead with a flat, high forehead is formed, while the upper orbital edges are flattened. This form is called “brachycephaly”. If the cases are severe, this is recognized by the tower shape of the head, it is pointed upward, which is called acrocephaly.
The neurological picture is nonspecific; ophthalmological and neurological phenomena become more pronounced at an earlier stage. Presumably, this has a connection with the large length of the seam.
Lambdoid craniosynostosis
The lambdoid suture, similar to the coronal suture, is divided into 1 part at the point of contact with the sagittal suture. Therefore, the child may have unilateral or bilateral damage.
In almost all cases, a unilateral nature of the lesion is observed in this form of craniosynostosis. A flattening of the occipital part appears, and occipital plagiocephaly is formed. It is very difficult to diagnose this synostosis, because unilateral fusion of the occiput in most cases is regarded by diagnosticians as “positional”, arising due to the forced position of the baby’s head on its side. This situation occurs when a child has a unilateral increase in muscle tone or is diagnosed with torticollis.
Synostosis in such cases can be distinguished by the fact that it practically does not change with age, although it is determined at the birth of the child. Positional plagiocephaly progresses significantly as the child undergoes physical therapy. Under the baby's hair, the deformation is only slightly visible; there are no obvious neurological manifestations. Therefore, lambdoid synostosis is difficult to diagnose in this group of diseases. However, early diagnosis and proper treatment are recommended because there is a risk of neurological impairment.
Syndromic craniosynostosis
This is the rarest and most complex group of congenital diseases of the craniofacial region. Surgical correction is difficult, and it is also very difficult to make a prognosis of mental and neurological development. In children, not only the growth of the bones of the facial skull is disrupted, but problems with breathing, vision, and cosmetic deformation occur.
The main symptom: brachycephaly due to premature synostosis of the coronary suture. The upper jaw is underdeveloped, therefore there is a depressed deformation of the face with exophthalmos and orbital hypertelloriema. The process of feeding a baby is disrupted because it is difficult for him to breathe, and the correct position of the jaws is also disturbed.
With syndromic craniosynostosis, the coronary and other sutures often overgrow, which leads to craniostenosis. Therefore, in addition to problems with breathing and nutrition, the child also suffers from neurological disorders. In such cases, early surgical intervention is important. Many children with syndromic craniosynostosis have a sharply enlarged large fontanelle, and there may be an expansion of the sagittal suture along its entire length. When diagnosing, this creates certain difficulties, because the enlarged fontanel is combined with premature healing of the sutures.
Patients with syndromic synostosis with unqualified care die before 12 months of life due to frequent and severe respiratory diseases, complications of which are pneumonia. If there is no surgical treatment for such patients, children later experience neurological and mental problems.
Prices
| Disease | Approximate price, $ |
| Prices for diagnosing migraine | 7 060 — 8 260 |
| Prices for diagnosing childhood epilepsy | 3 100 — 4 900 |
| Prices for brain shunting for hydrocephalus | 33 180 |
| Prices for treatment of Parkinson's disease | 58 600 |
| Prices for migraine treatment | 9 680 |
| Prices for the diagnosis of amyotrophic lateral sclerosis | 6 550 |
| Prices for diagnosing epilepsy | 3 520 |
| Prices for rehabilitation after a stroke | 78 300 — 82 170 |
| Prices for treatment of childhood epilepsy | 3 750 — 5 450 |
| Prices for treatment of multiple sclerosis | 4 990 — 17 300 |
| Disease | Approximate price, $ |
| Prices for diagnosing childhood arthritis | 2 000 — 3 000 |
| Prices for diagnosing childhood epilepsy | 3 100 — 4 900 |
| Prices for pediatric neurosurgery | 30 000 |
| Prices for treatment of childhood epilepsy | 3 750 — 5 450 |
| Prices for treatment of umbilical hernia in children | 9 710 |
| Disease | Approximate price, $ |
| Prices for pediatric neurosurgery | 30 000 |
| Prices for craniotomy | 43 490 — 44 090 |