Among the most common causes of disability in the population is pathology of the peripheral nervous system. Various factors are to blame for its occurrence: hereditary, metabolic, a consequence of taking medications, toxins entering the body, immune failures and unfavorable environmental conditions. Neuropathies, despite their prevalence and relative ease of diagnosis, remain on the list of complex diseases for which it is difficult to determine the true etiology. But this is precisely what plays a leading role in choosing an adequate course of treatment. The injection drug Nucleo CMF is recommended to buy for many lesions of the central and peripheral nervous system. For example, with radiculitis, neuritis of the facial nerve or intercostal neuralgia.
Types of polyneuropathy
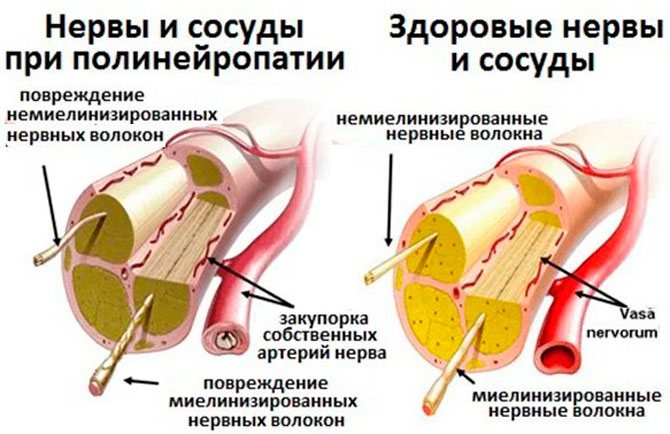
Polyneuropathy of the lower extremities is characterized by damage to the peripheral nerves, which entails sensitivity disturbances (it can decrease or increase) and deterioration of reflex functions.
There are many factors that provoke the development of the disease. Not only the treatment tactics used, but also some features in the clinical course of the disease depend on them. In total, there are 5 types of polyneuropathy of the lower extremities.
Sensory
The difficulty in diagnosing sensory polyneuropathy lies in its asymptomatic development in the initial stages. This is the insidiousness of pathology. Since, despite the absence of symptoms, it progresses and leads to irreversible consequences.
The first signs of the disease appear during the period when it reaches its peak. This manifests itself as sensory disorders in the form of numbness, burning, tingling, and a sensation of “pins and needles.”
Motor
It is developing rapidly. The main symptom is muscle weakness, up to complete inability to move the legs. Lack of therapy causes muscle atrophy, skin ulcers and infectious complications.
Sensorimotor
This form of the disease combines the clinical manifestations of sensory and motor polyneuropathy. At the same time, there is a decrease in sensitivity of the affected area and muscle weakness. Sensory polyneuropathy occurs in 70% of patients.
Vegetative
It manifests itself as a whole complex of symptoms, among which are:
- pale skin;
- excessive sweating;
- dizziness;
- loss of appetite;
- flatulence;
- bowel dysfunction (most often constipation);
- increased heart rate.
Signs of a disorder of the autonomic system accompany various diseases. Therefore, if they occur, you must immediately visit a doctor.
Mixed
This type of disease includes signs of all forms of polyneuropathy and manifests itself:
- decreased sensitivity;
- muscle weakness;
- motor dysfunction;
- autonomic disorders.
Symptoms
If the spinal column and spinal nerve roots are suddenly exposed to excessive force, acute radiculitis occurs, the main symptom of the disease will be vertebral neuralgia.
With degenerative and metabolic disorders, the process is chronic; pressure from an osteophyte, hernia, tumor or other formation is gradually exerted on the roots. Symptoms will gradually increase as the disease progresses.
It is worth understanding how radiculitis in various parts of the spine will manifest itself, since further diagnosis and treatment will depend on this. Inflammation of the roots of the cervical and lumbosacral regions, for example, will have a completely different clinical picture.
Diseases of the cervical spine are not uncommon, since this segment of the back is actively involved in holding the head when walking, running, sitting at a table, or working at a computer. The vertebrae in this part of the spine have a rather vulnerable structure, and at the same time they are in close interaction with important vessels and nerves.
If a spinal disease has led to inflammation of the nerve root in the cervical back, the following manifestations are likely to occur:
- Pain in the back of the head and neck, aggravated by exertion or prolonged immobile work.
- Pain in the shoulder blade, along the collarbone, in the area of the shoulder joint.
- Numbness, pain, loss of sensitivity in the hand. Radiculitis of the lower parts of the neck is manifested by disruption of the brachial plexus, which is responsible for the innervation of the upper limb.
- Loss of muscle strength in the arm.
- Headaches, migraines, dizziness are a sign of insufficient blood flow through the vertebral artery.
- Blood pressure disorders.
Most often, the disease manifests itself as neuralgia - pain at the exit site of the root and along the nerve fibers. Other signs appear if there is strong pressure on the nerve structures, or the inflammatory process becomes extensive.
The rarest form of radiculitis is damage to the thoracic region. The reason for this phenomenon is that a large number of vertebrae in the thoracic floor of the back take on part of the lost function, and the disease takes a long time to compensate.
In addition, in the thoracic region there are no such important structures as nerve plexuses or cauda equina, so only the spinal roots are involved in the process. Radiculitis of the thoracic region is manifested by the following symptoms:
- Pain in the thoracic part of the back, aggravated by exercise.
- Shootings along the chest, following the course of the ribs.
- Intercostal neuralgia can even mimic heart disease, occurring in the left side of the chest.
- Difficulty taking a deep breath due to chest pain.
Poor symptoms lead to the pathological process not being diagnosed for a long time. Dangerous diseases can be detected too late, so at the first symptoms you need to consult a doctor.
The most common location of radiculitis is the lumbosacral segment. This explains the large number of patients complaining of lower back pain.
The thing is that it is on the area of the lumbosacral floor that most of the load falls during active movements, lifting weights, and playing sports. Under the influence of these factors, degeneration occurs, which leads to aseptic inflammation of the nerve roots. Symptoms of lumbar radiculitis:
Radiculitis itself causes a lot of inconvenience, but it is also a manifestation of another disease. If the cause of neuralgia progresses, it may involve the nerve structure of the cauda equina, which is responsible for the innervation of the bladder and rectum.
Low back pain has been ignored by patients for a long time, but can be a symptom of a serious illness. It is necessary to consult a doctor in time for a full diagnosis of the disease.
Reasons for development
Various factors contribute to the development of polyneuropathy. These include:
- Diabetes. With this disease, the level of sugar in the blood increases, which leads to a change in its chemical composition. This entails a decrease in vascular density, deterioration in blood circulation and the process of supply of nutrients to nerve fibers. Nutritional deficiency leads to abnormalities in the myelin sheath of nerve endings, causing disorders in the peripheral system and the development of polyneuropathy of the lower extremities. It should be noted that this disease is diagnosed in 40% of diabetics.
- Lack of B vitamins. Vitamins from this group are directly involved in the construction of nerve fibers and the level of their conductivity. Their lack causes disturbances in the functioning of the peripheral system and the development of polyneuropathy.
- Long-term intoxication. Poisoning of the body can occur both due to the consumption of expired foods, alcoholic beverages and improper use of medications, and as a result of the development of infectious diseases (herpes, HIV, HPV). When intoxication is caused by chemicals, polyneuropathy develops rapidly and its first symptoms appear already 2-3 days after poisoning. In case of infectious and alcohol intoxication, disorders of the peripheral system are noted after 1-2 months.
- Injuries. Bone fractures, sprains and ruptures of ligaments lead to inflammation and swelling of tissues, and strong blows lead to hematomas, which compress nerve endings and blood vessels, disrupting blood circulation, causing the development of polyneuropathy. But it should be noted that not only injuries received from a blow or a fall provoke the disease. Its occurrence can also occur against the background of surgical interventions, intervertebral hernia, and pathological curvatures of the spine.
- Guillain-Barre syndrome. It is a consequence of infectious diseases and is characterized by changes in the functioning of the immune system, as a result of which the body begins to produce antibodies that destroy its own cells, including nerve endings.
- Hereditary predisposition. If parents have been diagnosed with polyneuropathy, there is a high risk of transmitting the disease to their children.
Polyneuropathy of the lower extremities can also develop in absolutely healthy women during pregnancy. The reason for this is the simultaneous influence of several factors:
- deficiency of B vitamins;
- inadequate reaction of the body to the fetus, leading to activation of autoimmune processes;
- long-term toxicosis;
- fetal pressure on the pelvic organs and nerve endings.
First manifestations
Depending on the form of the disease, the first signs of polyneuropathy can appear either a few days after damage to the peripheral system or after 1-2 months. First, the patient experiences unpleasant sensations in the feet (burning, tingling, numbness, a feeling of “pins and needles”). The symptoms then begin to spread upward, reaching the gluteal region.
In parallel with this, there is a violation of sensitivity. Moreover, it can not only decrease, but also increase. Painful sensations also occur. And the longer the disease progresses, the more pronounced the pain becomes. In the last stages of polyneuropathy, it occurs even with light touches.
The clinical picture is complicated by muscle weakness, “restless legs” syndrome (manifested by a feeling of burning feet, aching calves). And since with polyneuropathy, blood circulation is impaired, cracks, peeling, ulcers, and age spots are observed on the skin of the lower extremities. The patient may complain of cold feet.
Main features
Despite the fact that polyneuropathy has different forms, the clinical picture includes similar symptoms. It appears in the form:
- muscle weakness;
- deterioration or increase in sensitivity;
- disturbances of reflex functions;
- swelling of the legs;
- tremor;
- burning;
- coordination problems;
- excessive sweating (not only of the legs, but of the whole body);
- signs of tachycardia;
- deterioration of tissue regeneration (wounds, cracks, ulcers take a long time to heal).
The severity of the clinical picture depends on the type of polyneuropathy and the severity of its course. In some patients it appears suddenly, develops rapidly with severe symptoms, in others it can last for years and be accompanied by mild symptoms.
Treatment of diseases of the peripheral nervous system:
Treatment of these diseases includes medication, non-drug and surgical treatment. Drug therapy is aimed at correcting the underlying disease:
- Non-steroidal anti-inflammatory drugs (NSAIDs) are used to relieve pain.
- To normalize vascular tone and improve blood circulation, suitable vascular therapy is selected
- A course of vitamin therapy is prescribed to improve nerve conduction
- Recommended medications to normalize muscle tone
- and other medications, the selection of which is based on a specific pathology
Non-drug therapy includes the use of physiotherapeutic treatment methods, the selection of which depends on the specific pathology, the severity of the process and concomitant pathology:
- reflexology
- massage
- hirudotherapy
- ozone therapy
- osteopathy and manual therapy
As for surgical treatment methods, they are used in case of long-term persistent neurological defect and ineffectiveness of conservative therapy, or in acute conditions and there are absolute indications for surgical treatment.
For the best result from treatment, it is necessary to contact a neurologist for a face-to-face consultation as early as possible from the onset of the disease; the doctor will develop an individual treatment and examination regimen.
Diagnostics
Since polyneuropathy manifests itself with signs similar to those of other diseases, to make an accurate diagnosis it is necessary to undergo a comprehensive examination. But before prescribing computer and laboratory tests, the neurologist examines the medical history, conducts an examination of the patient and several tests to identify lesions and the degree of impairment of reflex functions.
After this, laboratory tests are prescribed:
- UAC;
- OAM;
- blood and urine tests to determine sugar levels;
- blood chemistry.
Computer diagnostics includes:
- electroneuromyography;
- neurophysiological research.
These methods make it possible to accurately assess the state of the peripheral system, determining not only the affected areas, but also the speed of signal transmission by nerve endings. In case of complicated polyneuropathy, a nerve biopsy may be required.
And in order to establish the cause of the disease and select treatment, diagnosis also includes:
- Ultrasound;
- MRI;
- CT;
- ECG;
- radiography.
Difficulties of therapy for lesions of the PNS
In truth, any peripheral nerve disease is still difficult to treat. Traditional therapy can only do the most to eliminate the symptoms of the disease. The response of the PNS to pathology is quite limited and when the nerve is damaged, the following processes can occur:
- Crossing a nerve is a Wallerian degeneration;
- Axonopathy – axon degeneration;
- Myelinopathy – segmental demyelination;
- Neuronopathy is a primary cell damage.
In order to promote the physiological regeneration of peripheral nerves in such conditions, special active components are required - pyrimidine nucleotides. It is these substances that have become increasingly used in the treatment of various lesions of the nervous system. Preparations based on such components, for the most part, were developed in European pharmaceutical companies and are almost never found on the CIS market. The issues of certification of drugs for the treatment of PNS diseases in our country are acute, but there is not much movement towards improving the situation. Therefore, it is possible to obtain such medicines only through intermediary companies; for example, Nucleo ampoules can only be purchased in Moscow through Internet sites.
General therapy
Polyneuropathy is a serious disease that affects the peripheral systems. During its development, nerve fibers are destroyed and it takes a long time to restore them. First of all, therapy is aimed at eliminating the provoking factor. If it is not possible to completely stop it, then every effort is made to minimize its effect on the body. For example:
- for diabetes mellitus, a course of insulin therapy is prescribed to help normalize blood sugar levels;
- for infectious diseases, antibacterial drugs, antiviral agents, and immunomodulators are used;
- in case of deficiency of B vitamins, intramuscular injections are prescribed (the drug is selected individually, depending on the type of the missing vitamin);
- For pathologies of the endocrine system, hormonal agents are used to restore the balance of hormones in the body.
If it is not possible to stop the cause of the development of polyneuropathy, all therapeutic measures are aimed at eliminating the symptoms of the disease. For this purpose, painkillers, metabolites, and drugs that improve the conductivity of nerve fibers are prescribed. Additionally, diet, exercise therapy, physiotherapeutic procedures, acupuncture, etc. are used.
Conduction of impulses along nerve fibers.
Action potentials (excitation impulses) have the ability to propagate along nerve and muscle fibers. Potentials can be local; they propagate over short distances of 1-2 mm with attenuation (decrement) and pulses. Pulse potentials propagate without decrement over considerable distances - up to several tens of centimeters. Local potentials arise in response to the action of a subthreshold stimulus, for example, on the membrane of a receptor cell.
The transmission of information over long distances within the nervous system is carried out using nerve impulses along the axons of neurons. A prerequisite for the conduction of a nerve impulse is the presence of potential-sensitive ion channels along the entire length or in limited but repeating sections of the fiber.
Depending on the location and concentration of ion channels in the fiber membrane, there are two ways of conducting a nerve impulse.
1. Continuous conduction of the nerve impulse occurs in non-myelinated fibers and is explained by the uniform distribution of the potential of sensitive ion channels involved in the generation of action potentials.
The resulting AP ensures the opening of potential-gated Na channels in the adjacent section of the nerve fiber membrane and the movement of Na+ ions into the fiber, which ensures the development of a critical level of depolarization in the adjacent section of the nerve fiber and the emergence of a new AP.
2. Saltatory conduction of a nerve impulse (NP) occurs in myelin fibers, since their potential-sensitive ion channels are localized only in areas of the membrane of the nodes of Ranvier, where their density reaches 12,000 per 1 µm2. In the area of internodal segments, which have high insulating properties, there is no potential for sensitive channels, as a result of which the membrane of the axial cylinder there is practically inexcitable. Therefore, an AP arising in one node of Ranvier spreads through the internodal segment to the adjacent node, depolarizes the membrane to a critical level and causes the occurrence of an action potential.
Saltatory conduction of nerve impulses is an evolutionarily later mechanism that first appeared in vertebrates in connection with the myelination of nerve fibers. It has two important advantages compared to the continuous excitation mechanism:
— more economical in terms of energy consumption;
- excitation is carried out at a higher speed (up to 120 m/s) than in unmyelinated fibers (0.5-2.0 m/s).
All features of the spread of excitation in the central nervous system are explained by its neural structure: the presence of chemical synapses, multiple branching of neuron axons, and the presence of closed neural pathways.
In addition, there are several types of excitation propagation:
1. Irradiation (divergence) of excitation in the central nervous system, which is explained by the branching of axons and the presence of interneurons, the axons of which also branch. Divergence expands the scope of each neuron. One neuron, sending impulses to the cerebral cortex, can participate in the excitation of up to 5000 neurons.
2.
Convergence of excitation is the convergence of several nerve impulses traveling along different paths to the same neuron.
3. Circulation of excitation along closed neural circuits occurs as a result of the closure of a group of neurons into a ring structure. The circulation of excitation is one of the causes of the aftereffect phenomenon. It is believed that the circulation of excitation in closed neural circuits is the most likely mechanism of the phenomenon of short-term memory. Circulation of excitation is possible in a chain of neurons and within one neuron as a result of contacts of the branches of its axon with its own dendrites and body.
38. Sheaths of the spinal cord. The spinal cord is covered with three membranes: the outer - hard, middle - arachnoid, internal - vascular. The hard shell of the spinal cord consists of dense, fibrous connective tissue, which starts from the edges of the occipital foramen in the form of a bag, descends to the level of the 2nd sacral vertebra, and then it goes as part of the final filament, forming the outer layer, to the level of the 2nd coccygeal vertebra. The arachnoid membrane of the spinal cord is a thin and transparent, avascular, connective tissue layer located under the dura mater. The choroid of the spinal cord is tightly adjacent to the substance of the spinal cord . It consists of loose connective tissue, rich in blood vessels that supply blood to the spinal cord. There are three spaces between the membranes of the spinal cord: above the dura mater - the epidural space; under the dura mater - subdural space; subarachnoid. The epidural space is located between the dura mater and the periosteum of the spinal canal. It is filled with fatty tissue, lymphatic vessels and venous plexuses, which collect venous blood from the spinal cord, its membranes and the spinal column. The subdural space is a narrow gap between the dura mater and the arachnoid. The subarachnoid space, located between the arachnoid and pia mater, is filled with cerebrospinal fluid. In the area of the foramen magnum, it communicates with the subarachnoid spaces of the brain, which ensures the circulation of cerebrospinal fluid. Downwards, the subarachnoid space expands, surrounding the cauda equina. At the top, the spinal cord is connected to the brain, and at the bottom, its terminal filament fuses with the periosteum of the coccygeal vertebrae. For fixation of the spinal cord, the formation of the epidural space (fatty tissue, venous plexus), which acts as an elastic lining, and the cerebrospinal fluid in which the spinal cord is immersed are important.
39. Laws and types of initiation.
The conduction of nerve impulses along neuron fibers is governed by certain laws:
Law 1 : the nerve impulse spreads in both directions from the site of irritation.
Law 2 : conduction of a nerve impulse along a fiber occurs in isolation and does not spread to parallel fibers. The explanation for this law is that the axolemma has a very high resistance and does not pass current loops to unexcited fibers located nearby. Isolated conduction ensures high accuracy of the regulatory activity of the central nervous system.
Law 3 : the speed of excitation along a nerve fiber is determined by its diameter. Hence the consequence: the thicker the nerve fiber, the greater the speed of the nerve impulse along this fiber.
Law 4 : the nerve retains the ability to conduct excitation for 6-8 hours of continuous stimulation (N.E. Vvedensky’s law, 1883).
Law 5 : the action of substances that block the operation of ion channels, without compromising the integrity of the nerve fiber, causes a state of reversible parabiosis.
In addition, there are several types of excitation propagation:
1. Irradiation (divergence) of excitation in the central nervous system, which is explained by the branching of axons and the presence of interneurons, the axons of which also branch. Divergence expands the scope of each neuron. One neuron, sending impulses to the cerebral cortex, can participate in the excitation of up to 5000 neurons.
2.
Convergence of excitation is the convergence of several nerve impulses traveling along different paths to the same neuron. The phenomenon of convergence of excitation propagation was described by E. Sherrington, so the phenomenon was called the Sherrington funnel principle or the principle of a common final path.
3. Circulation of excitation along closed neural circuits occurs as a result of the closure of a group of neurons into a ring structure. The circulation of excitation is one of the causes of the aftereffect phenomenon. It is believed that the circulation of excitation in closed neural circuits is the most likely mechanism of the phenomenon of short-term memory. Circulation of excitation is possible in a chain of neurons and within one neuron as a result of contacts of the branches of its axon with its own dendrites and body.
40.Segmental structure of the spinal cord.
A neural segment is a transverse segment of the spinal cord and the associated right and left spinal nerves. In other words, this is a section of the spinal cord corresponding to two pairs of spinal roots (two anterior and two posterior). The spinal cord has 31–33 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1-3 coccygeal segments. Each segment of the spinal cord corresponds to a specific area of the body that receives innervation from this segment. The segments are designated by initial letters indicating the region (part) of the spinal cord and numbers corresponding to the serial number of the segment: cervical segments ( segmentacervicalia
) – CI–CVIII, thoracic segments (
segmentathoracica
) – ThI–ThXII, lumbar segments (
segmentalumbalia
) – LI–LV, sacral segments (
segmentasacralia
) – SI–SV, coccygeal segments (
segmentacoccygeal
) – CoI–CoIII. The length of the spinal cord is significantly less than the length of the spinal column, therefore the serial number of any segment of the spinal cord does not correspond to the serial number of the vertebra. Each spinal nerve begins with two roots, one of which emerges from the anterior sulcus (motor root), and the other from the posterior sulcus (sensitive root). Bundles of roots, leaving the brain, are directed to the intervertebral foramina. Here the dorsal root forms a swelling - the spinal ganglion, and then connects with the anterior root into one mixed nerve.
The mixed nerve is divided into 4 branches: dorsal, abdominal, connective, meningeal. The dorsal branch goes to the dorsal side of the body and innervates the deep muscles of the back and corresponding areas of the skin. The abdominal branch (thicker) is located in front, it innervates the muscles and skin of the abdominal and lateral surfaces of the body, as well as the limbs. The connective tissue branch connects the spinal cord with the sympathetic nodes (ganglia) from the I thoracic to the II lumbar nerve. The thin meningeal branch returns to the brain through intervertebral foramen and innervates the membranes of the spinal cord and the wall of the spinal canal. Approaching the innervated organs, these branches branch and end with terminal fibers in the perceiving - receptor, or working - effector organs. Thus, each spinal nerve is mixed, since it contains both sensory and motor fibers.
41. Structural organization of chemical and electrical synapses. The basic structural and functional unit of the nervous system is the neuron. A huge number of structural units in the nervous system are united by intercellular contacts, which at the end of the 19th century the outstanding physiologist Charles Sherrington called synapses. Synapses ensure the continuity of information transmission in the nervous system; they mediate signal transmission from the end of the axon to the effector cell - a neuron, muscle fiber or secretory cell. A synapse is a structure that ensures the transmission of excitatory or inhibitory influences between two excitable cells. Depending on the method of transmission of nerve impulses, synapses can be chemical or electrical (electrotonic). Both methods of synaptic transmission are present in the nervous system of lower and higher animals, but in higher vertebrates the chemical method of information transmission predominates. Depending on the nature of the signal, synapses can be excitatory or inhibitory. First of all, let's consider the structure of a chemical synapse. A chemical synapse is the structure of the nerve ending of an axon, its diameter is no more than 1 micron. Each synapse is securely closed by special glial cells. Chemical synapses transmit a nerve impulse to another cell with the help of special biologically active substances - neurotransmitters[8] located in synaptic vesicles. The obligatory structures of a synapse are: -
presynaptic ending – i.e. a separate section of the membrane of a nerve cell that transmits an impulse. In this area, calcium channels are localized, promoting the fusion of synaptic vesicles with the presynaptic membrane and the release of the transmitter into the synaptic cleft; - synaptic cleft - the space between the pre- and postsynaptic membranes. The synaptic cleft of a chemical synapse has a width of 20-50 nm, it contains intercellular fluid and mucopolysaccharide substance in the form of bridges, which provide pre- and postsynaptic membranes; - the postsynaptic membrane is a section of the cell plasmalemma equipped with receptor zones for the perception of the corresponding neurotransmitter. Presynaptic ending formed along the branching of the axon. The main structural elements of the presynaptic terminal are synaptic vesicles, ribosomes, mitochondria and neurofilaments. The shape and contents of synaptic vesicles are related to the function of the synapse. They are round transparent with a diameter of 30-50 nm and dark bubbles with a diameter of 50-90 nm. Each vesicle contains between 1,000 and 10,000 molecules of a chemical involved in nerve signal transmission. Small vesicles, as a rule, are filled with acetylcholine molecules (cholinergic synapses) as a mediator; large vesicles contain the mediator norepinephrine (adrenergic synapses). To synthesize the mediator, enzymes are needed that are formed on ribosomes in the body of the neuron. The presynaptic membrane ensures the release of the transmitter into the synaptic cleft through exocytosis. In the work of chemical synapses, several important features of excitation can be identified: 1. Unilateral conduction of excitation - in the direction from the presynaptic ending towards the postsynaptic membrane. 2. Slow signal transmission, which is 0.2-0.5 ms. 3. Low lability, i.e. the frequency of transmission of nerve impulses per second is reduced by 5-6 times in comparison with the transmission of impulses along the axon. 4. The conductivity of chemical synapses changes greatly under the influence of biologically active substances (medicines, blockers and stimulants).
42. Conducting tracts and nuclei of the spinal cord. The totality of processes of nerve cells of the gray matter forms three systems of bundles (or pathways) of the spinal cord in the cords of the spinal cord:
1) short bundles of associative fibers connecting segments of the spinal cord located at different levels;
2) ascending (afferent, sensory) bundles heading to the centers of the cerebrum and cerebellum;
3) descending (efferent, motor) bundles going from the brain to the cells of the anterior horns of the spinal cord.
In the white matter of the anterior cords there are predominantly descending pathways, in the lateral cords there are both ascending and descending pathways, and in the posterior cords there are ascending pathways.
Anterior cord
1. The anterior corticospinal (pyramidal) motor tract contains processes of giant pyramidal cells. The pathway transmits impulses of motor reactions from the cerebral cortex to the anterior horns of the spinal cord.
2. The reticular-spinal tract conducts impulses from the reticular formation of the brain to the motor nuclei of the anterior horns of the spinal cord. It is located in the central part of the anterior cord.
3. The anterior spinothalamic tract is located slightly anterior to the reticular spinal tract. Conducts impulses of tactile sensitivity (touch and pressure).
4. The tegmental spinal tract connects the subcortical centers of vision (superior colliculi of the midbrain roof) and hearing (inferior colliculi) with the motor nuclei of the anterior horns of the spinal cord. The presence of such a tract allows for reflex protective movements during visual and auditory stimulation.
5. The vestibulospinal tract is located on the border of the anterior cord with the lateral cord. The fibers of this pathway go from the vestibular nuclei of the VIII pair of cranial nerves, located in the medulla oblongata, to the motor cells of the anterior horns of the spinal cord.
The lateral cord of the spinal cord contains the following pathways.
Ascending paths.
1. The posterior spinocerebellar tract (Flexig's bundle) conducts impulses of proprioceptive sensitivity.
2. The anterior spinocerebellar tract (Gowers' bundle), also carrying proprioceptive impulses to the cerebellum.
3. The lateral spinothalamic tract is located in the anterior sections of the lateral cord and conducts impulses of pain and temperature sensitivity.
Descending paths.
The descending fiber systems of the lateral cord include the lateral corticospinal (pyramidal) and red nucleus-spinal (extrapyramidal) pathways.
4. The lateral corticospinal (pyramidal) tract conducts motor impulses from the cerebral cortex to the anterior horns of the spinal cord.
5. The red nuclear spinal tract is a conductor of impulses for automatic (subconscious) control of movements and tone of skeletal muscles and goes to the anterior horns of the spinal cord.
The posterior cord at the level of the cervical and upper thoracic segments of the spinal cord is divided into two bundles by the posterior intermediate sulcus. The medial one is directly adjacent to the posterior longitudinal groove - this is a thin bundle (Gaulle's bundle). Its lateral location is a wedge-shaped bundle (Burdach's bundle), adjacent on the medial side to the posterior horn.
The thin bundle consists of longer conductors running from the lower torso and lower extremities to the medulla oblongata. The thin and wedge-shaped bundles are bundles of proprioceptive sensitivity (articular-muscular sense), which carry information about the position of the body and its parts in space to the cerebral cortex.
43.Features of the morphology and physiology of electrical synapses.
Electrical, or electrotonic, synapses are relatively rare in the mammalian nervous system. In the area of such synapses, the cytoplasms of neighboring neurons are connected by gap-like junctions, ensuring the passage of ions from one cell to another, and, consequently, the electrical interaction of these cells. Electrical synapses have a synaptic gap that is an order of magnitude smaller than that of chemical synapses. They conduct signals in both directions without synaptic delay. Signal transmission in such a synapse is not blocked by a lack of calcium, they are insensitive to pharmacological drugs, poisons, and are practically not fatigued, like all nerve fibers. The contacting membranes of neurons are connected to each other by semi-channels of a protein nature, they are called connexons ( connection
- connection). The connexon sections have a very low resistivity, which ensures high electrical conductivity.
Electrical synapses are represented in the reticular formation of the brain, the trigeminal nucleus, the vestibular nucleus and the olives of the medulla oblongata. The functional role of electrical synapses is to carry out urgent signal transmission that synchronizes the electrical activity of a group of neurons, for example, a group of motor neurons during the jumping movements of a frog or the swimming movements of a fish.
44.The mechanism of signal transmission in synapses.
The autonomic nervous system is divided into sympathetic and parasympathetic parts[9]. The sympathetic part of the autonomic nervous system has a stimulating effect on the heart. When it is irritated, we observe an increase in heart rate, increased blood flow, increased oxygen exchange in the myocardium, etc. The sympathetic effect on the heart is called the positive chronotropic effect.
.
The parasympathetic part of the autonomic nervous system has the opposite effect, causing a decrease in heart rate, i.e. causes a negative chronotropic effect
. Physiologist Otto Levy[10] found that when the sympathetic nerve of an isolated frog's heart is irritated, a substance is released that can stimulate cardiac activity in another frog. When the cardiac branch of the vagus nerve is irritated, a substance is formed that inhibits the activity of the heart. Subsequently, it was shown that the substance causing the negative chronotropic effect is broken down by the enzyme acetylcholinesterase and is identical to acetylcholine. Under the influence of acetylcholine, the permeability of the postsynaptic membrane of conducting fibers for potassium ions increases and their permeability for calcium ions decreases. There is an increase in the output of potassium ions from the cells and a decrease in the entry of calcium ions. This leads to hyperpolarization of membranes and a decrease in their excitability. In the case of a positive chronotropic effect, another mediator acts - norepinephrine, which activates β-adrenergic receptors that increase the permeability of the postsynaptic membrane for sodium and calcium ions, and also accelerates the metabolism and formation of ATP with an increase in the breakdown of glycogen in cardiac fibers. An increase in permeability to sodium ions leads to depolarization of the postsynaptic membrane and excitation of the muscle cells of the heart. The facts established by Otto Lewy served as the basis for the creation of the theory of chemical transmission of nervous excitation. According to the theory, when a transmitter comes into contact with the receptors of the postsynaptic site of the synaptic apparatus, the ionic permeability of the postsynaptic (receiving) membrane changes. A change in ionic permeability causes a change in the electrochemical potential: an increase in the concentration gradient leads to hyperpolarization (inhibition) of the postsynaptic membrane, and a decrease in the gradient leads to the development of depolarization of the postsynaptic membrane and excitation of the nerve cell. The mediator, released in the presynaptic endings under the influence of incoming nerve impulses, interacts with a specific protein -receptor of the postsynaptic membrane and forms a temporary complex compound with it. For example, the protein with which acetylcholine interacts is called a cholinergic receptor, adrenaline or noradrenaline is an adrenergic receptor. Substances that have an effect on the effector organ similar to the action of a particular mediator are called mimetics, and substances that weaken the effect of the mediator are lytics. The N-anticholinergic tubacurarine is an alkaloid that blocks nerve impulses that control muscles. This blockage leads to muscle paralysis: first of all, the fingers and toes and eyelids stop working, then the nerve endings responsible for vision and hearing are paralyzed, then paralysis affects the face, neck, arms and legs, and finally death occurs from respiratory paralysis . This anticholinergic blocks the interaction of acetylcholine with cholinergic receptors. One of the important inhibitory mediators is GABA. There are two types of GABA receptors on the postsynaptic membrane: GABA-A (opens channels for chloride ions) and GABA-B (opens channels for K+ or Ca++, depending on the cell type). Bicuculline is a well-known GABA antagonist. It passes well through the blood-brain barrier and has a strong effect on the body even in small doses, causing convulsions and death. GABA is found in a number of neurons of the cerebellum (Purkinje cells, Golgi cells, basket cells), hippocampus (basket cells), olfactory bulb and substantia nigra. Another well-known inhibitory transmitter is glycine. Glycinergic neurons are found mainly in the spinal cord and medulla oblongata. It is believed that these cells act as inhibitory interneurons.
45. Structure of the spinal cord . The spinal cord is a long, cylindrical cord, flattened from front to back, located in the spinal canal. At the top it passes into the medulla oblongata, at the bottom it ends in a pointed medullary cone. The apex of the conus medullaris of the spinal cord continues into the thin filum terminale. The length of the spinal cord in an adult is on average 43 cm (in men - 45 cm, in women - 41-42 cm), weight - about 34-38 g, which is approximately 2% of the weight of the brain. In the cervical and lumbosacral parts of the spinal cord has two thickenings - the cervical and lumbosacral thickening. The formation of thickenings is explained by the fact that the upper and lower extremities are innervated from the cervical and lumbosacral parts of the spinal cord. These sections of the spinal cord contain more nerve cells and fibers than other sections. The external structure of the spinal cord is considered relative to the anterior and posterior surfaces. On the anterior surface of the spinal cord, the anterior median fissure is visible, which protrudes deeply into the tissue of the spinal cord. On the posterior surface is the posterior median groove. They are the boundaries that divide the spinal cord into two symmetrical halves. The anterior lateral groove extends away from the anterior fissure. It serves as the exit point for the anterior (motor) roots of the spinal nerves and the boundary on the surface of the spinal cord between the anterior and lateral cords. On the posterior surface of the spinal cord is the posterior lateral sulcus - the site of penetration of the posterior (sensitive) roots of the spinal nerves into the spinal cord. This groove serves as the boundary between the lateral and posterior funiculi.
The anterior root consists of processes of motor (motor) nerve cells located in the anterior horn of the gray matter of the spinal cord. The dorsal root is sensitive, represented by a set of central processes of neurons penetrating the spinal cord, the bodies of which form the spinal ganglion, which lies outside the spinal cord at the junction of the dorsal root with the anterior one. Throughout the entire length of the spinal cord, 31–33 pairs of roots emerge from each side. The anterior and posterior roots join to form the spinal nerve.
The spinal cord consists of nerve cells and fibers of gray matter, which in cross section looks like the letter H or a butterfly with spread wings. On the periphery of the gray matter there is white matter formed only by nerve fibers. The gray matter of the spinal cord contains a central canal. It is a remnant of the neural tube cavity and contains cerebrospinal fluid. The upper end of the canal communicates with the fourth ventricle of the brain, and the lower, slightly expanding, forms a blindly ending terminal ventricle (Krause’s ventricle). The walls of the central canal of the spinal cord are lined with ependyma, around which there is a central gelatinous (gray) substance. Ependyma is a dense layer of neuroglial cells that perform demarcation and support functions. On the surface facing the cavity of the central canal there are numerous cilia that facilitate the flow of cerebrospinal fluid in the canal. Long branching processes extend into the brain tissue from ependymocytes, performing a supporting function.
The gray matter along the spinal cord to the right and left of the central canal forms symmetrical gray columns. Each column of gray matter has its front part, the anterior column, and its back part, the posterior column. At the level of the lower cervical, all thoracic and two upper lumbar segments of the spinal cord, the gray matter on each side forms a lateral protrusion - the lateral column. In other parts of the spinal cord (above the VIII cervical and below the II lumbar segments) there are no lateral columns.
In a cross section of the spinal cord, the columns of gray matter on each side have the appearance of horns. There is a wider anterior horn and a narrow posterior horn. The lateral horn corresponds to the lateral intermediate (vegetative) column of the gray matter of the spinal cord. The anterior horns contain large nerve root cells - motor (efferent) neurons. The posterior horns of the spinal cord are represented predominantly by small cells. The gray matter of the dorsal horns of the spinal cord is heterogeneous. Anteriorly, a gelatinous substance consisting of small nerve cells is secreted. The processes of nerve cells of the jellylike substance communicate with neighboring segments and are represented mainly by glial cells. The cells of all nuclei of the dorsal horns of the gray matter are interneurons. Neurites arising from the nerve cells of the dorsal horns travel in the white matter of the spinal cord to the brain.
The intermediate zone of gray matter of the spinal cord is located between the anterior and posterior horns. Here, from the VIII cervical to the II lumbar segment, there is a protrusion of gray matter - the lateral horn. In the medial part of the base of the lateral horn is the thoracic nucleus, consisting of large nerve cells. This nucleus extends along the entire posterior column of gray matter in the form of a cellular cord (Clark's nucleus).
In the lateral horns there are centers of the sympathetic part of the autonomic nervous system in the form of several groups of small nerve cells, united in the lateral intermediate (gray) substance and the central intermediate (gray) substance, the cell processes of which participate in the formation of the spinocerebellar tract. At the level of the cervical segments of the spinal cord, between the anterior and posterior horns, and at the level of the upper thoracic segments, between the lateral and posterior horns, the reticular formation is located in the white matter.
Drug treatment
For polyneuropathy, drugs are used that promote:
- increased blood circulation;
- normalization of metabolism;
- restoration of sensitivity and reflex functions.
Metabolic drugs
Medicines from these groups are the basis for the treatment of polyneuropathy. They combat free radicals, improve nutrition of nerve fibers, increase blood flow, and normalize regeneration and metabolism. Thus, it turns out that just one drug can have the effect of several medications at once.
Metabolic agents that contribute to the treatment of polyneuropathy of the lower extremities include:
- Thioctic acid;
- Actovegin;
- Instenon;
- Cytochrome C;
- Mexidol;
- Calcium pantothenate;
- Cerebrolysin.
Usually preference is given to one drug. Its choice depends on the cause of the development of polyneuropathy. For example, if it is a consequence of diabetes, Thioctic acid is used, and for obliterating atherosclerosis, Actovegin is used. Metabolic drugs are taken in courses of 1 month or more.
Vitamins
Therapy for polyneuropathy of the lower extremities is not complete without the use of B vitamins. Most often, vitamins B1, B6, B12 are used for this disease. As a rule, they are used simultaneously, as they interact well with each other and ensure the restoration of the peripheral nerve sheaths. But besides this, B vitamins reduce pain and have an antioxidant effect, which has a beneficial effect on the condition of blood vessels and blood circulation.
Doctors give their preference to combination products that contain all 3 vitamins. At the very beginning of treatment, drugs are used in the form of solutions for intramuscular injections, then they switch to tablet forms.
The most commonly used injections are:
- Milgamma;
- Combilipen;
- Compligam B;
- Vitaxon;
- Vitagamma.
In addition to vitamins, these products contain lidocaine, which enhances the analgesic effect. Lidocaine-free injections Neuromultivit and Neurobion can also be used for injections. Injections are given 3 times a day for 10 days. The drugs are then taken orally in tablet form for at least 1 month.
Painkillers
The pain that occurs with polyneuropathy significantly worsens the quality of life of patients. Sometimes, because of it, they cannot walk independently or sleep normally. In such cases, painkillers are prescribed. These include anticonvulsants, antidepressants, local anesthetics, and opioid medications. The use of banal painkillers such as Analgin and Pentalgin is not used for polyneuropathy, since they do not have the desired effect in this disease.
Among the anticonvulsants, the most commonly used are:
- Tebantin;
- Gabagamma;
- Catena;
- Lyrics.
Among antidepressants, preference is given to Amitriptyline. Lidocaine is used as a local anesthetic. If the use of these medications does not help relieve pain, they resort to prescribing opioids, which include Tramadol.
Drugs that improve the conduction of nerve impulses
If persistent sensory disturbances and muscle weakness are observed with polyneuropathy, anticholinesterase drugs are used to improve neuromuscular conduction). These medications work even in cases where there are defects in the nerve sheaths. They ensure the passage of impulses through entire sections of nerve endings, which increases muscle strength and returns sensitivity.
Among such drugs in the treatment of polyneuropathy, the following are most often used:
- Neuromidin;
- Amiridine;
- Aksamon;
- Ipigrix.
Peptides in a spray for the prevention and treatment of stroke
The drug Rekovin INS is designed specifically for the prevention and treatment of pre-stroke conditions , rehabilitation after a stroke . In the first case, with timely and regular use, it relieves vascular spasm, stopping an impending stroke; in the second, when the disease has occurred, it eliminates and treats all signs of a stroke , such as slurred speech, numbness of the limb, facial asymmetry. It is recommended to take for people with hypertension and headaches, for everyone who is at risk for a stroke, for everyone who has already had it before - keep it on hand as an emergency aid, and it is better to use it - 1-2 times a day for 3-4 pressing. The drug will restore blood circulation to the brain, revive already dead capillaries, the effect can surprise even practicing doctors. Without guile or unnecessary modesty: this may be your only opportunity to restore and return to normal life a loved one who has suffered a stroke.