tags:
Aspiration, Behavior, Appetite, Need, Suppression, Activity, Impairment, Disorder - behavioral disorders. Quantitative changes and distortions of drives are distinguished.
Hyperbulia
is
a general increase in will and drives, affecting all the basic drives of a person.
- increased appetite
- hypersexuality...
!!! The simultaneous increase in drives and will, as a rule, does not allow
patients commit
sexual
. Usually they do not pose a danger; they can disturb others with their intrusiveness, fussiness, behave carelessly, and misuse property.
- Manic syndrome.
Hypobulia
–
a general decrease in will and drives; all basic drives are suppressed, including physiological ones.
- decreased appetite
- decreased sexual desire
- no need for communication, are burdened by the presence of strangers and the need to maintain a conversation, ask to be left alone
— immersed in the world of their own suffering and cannot show concern for loved ones. Suppression of the instinct of self-preservation - suicide attempts
.
- a feeling of shame for one’s inaction and helplessness.
- Depressive syndrome (suppression of impulses during depression is a temporary, transient disorder. Relieving an attack of depression leads to renewed interest in life and activity).
Abulia
– a sharp decrease in will; no suppression of physiological drives is observed.
- laziness and lack of initiative
- normal need for food
- distinct sexual desire
They are satisfied in the simplest, not always socially acceptable, ways.
20 pp., 9613 words
General characteristics of a person’s motivational sphere
32 Motivation – 1. is a mental formation that reveals the reasons for a person’s behavior, encourages and directs his activity; 2. a system of factors that determine behavior (needs, motives, goals, interests, desires, intentions, aspirations); 3. characteristics of the process that stimulates and maintains behavioral activity at a certain level. Fifth-grader Andrey constantly...
- do not need communication, entertainment, can spend all days inactive
- are not interested in events in the family and in the world
Persistent negative disorder, together with apathy - apathetic-abulic syndrome (end states in schizophrenia).
Perversions of drives (parabulia).
-
perversion of appetite, sexual desire, desire for antisocial behavior, self-harm.
Parabulia is not considered as an independent disease, but is only a symptom.
Causes: gross intellectual impairment ( mental retardation, total dementia
), various forms of schizophrenia (
both in the initial period and at the final stage with the so-called schizophrenic dementia
), as well as psychopathy (
persistent personality disharmony)
;
manifestation of metabolic disorders ( eating inedible things during anemia or pregnancy
), as well as endocrine diseases (
increased appetite in diabetes, hyperactivity in hyperthyroidism, abulia in hypothyroidism, sexual behavior disorders due to an imbalance of sex hormones
).
| Name of disorder | Nature of manifestation |
| Pyromania | The desire to commit arson |
| Kleptomania | Pathological theft |
| Trichotillomania | The urge to pull out one's hair |
| Pica (pica) | The desire to eat inedible things (as a variation, coprophagia - eating excrement) |
| Dipsomania | Craving for alcohol |
| Dromomania | The desire to wander |
| Homicidomania | Senseless desire to commit murder |
| Suicidemania | Suicidal impulse |
| Oniomania | The urge to make (often unnecessary) purchases |
| Anorexia nervosa | The desire to limit oneself in food, to lose weight |
| Bulimia | Binges of overeating |
| Transsexualism | The desire to change gender |
| Transvestism | The desire to wear clothes of the opposite sex |
| Paraphilias, including: | Sexual preference disorders |
| fetishism | Obtaining sexual satisfaction from contemplating intimate clothing items |
| exhibitionism | Passion for nudity |
| voyeurism | Passion for peeping on nudes |
| pedophilia | Attraction to minors in adults |
| sadomasochism | Achieving sexual gratification by inflicting pain or mental suffering |
| homosexuality | Same-sex attraction |
By degree:
Obsessive (obsessive) attraction -
the emergence of desires that the patient can control in accordance with the situation. Attractions that clearly diverge from the requirements of ethics, morality and legality are in this case never implemented and are suppressed as unacceptable.
Refusal to satisfy an instinct gives rise to strong feelings; against your will, thoughts about an unfulfilled need are constantly stored in your head. If it is not clearly antisocial in nature, the patient carries it out as soon as possible.
- Obsessive-phobic syndrome
- Mental dependence on psychotropic drugs
Compulsive drive
- a more powerful feeling, comparable in strength to hunger, thirst, and the instinct of self-preservation.
Patients are aware of the perverted nature of the drive, try to restrain themselves, but when the need is unsatisfied, an unbearable feeling of physical discomfort arises - the pathological need occupies such a dominant position that the person quickly stops the internal struggle and satisfies his drive, even if this is associated with gross antisocial actions and the possibility of subsequent punishment ( repeated violence, serial murders...
)
- The desire for drugs during withdrawal syndrome in those suffering from alcoholism and drug addiction (physical dependence syndrome)
- Manifestation of psychopathy
Impulsive attraction
- an irresistible urge to commit certain actions, completely taking over the mind with the simultaneous suppression of any other aspirations, ideas, desires, devoid of explanation of the motives of the actions.
They appear suddenly and are immediately, as if automatically, realized. Memory
information about him and the circumstances surrounding him
are completely preserved
.
Confronting the emerging disorder, understanding its unnaturalness, brings impulsive attraction closer to obsessive attraction for some time. However, subsequently the struggle of motives disappears and the impulsive attraction is realized. After realizing an impulsive desire, they often experience a feeling of sharp mental relief; some patients report the appearance of peace of mind. At the same time, a decline in physical and mental tone may occur.
Impulsive drives occur in the form of a single episode
.
In some cases they are repeated repeatedly and in a stereotypical form
.
- organic diseases of the brain (encephalitis, Pick's disease, progressive paralysis) - suddenly appear and are immediately realized
Emotional disorders
- excessive expression of a person’s natural emotions or disruption of their dynamics.
Hypotymia
is
a persistent, painful low mood (
sadness, melancholy, depression)
.
- Amazing durability
— Extremely pessimistic assessment of one’s condition and existing prospects
- Inability to experience joy.
Gravity:
from mild sadness, pessimism to a deep physical (vital) feeling, experienced as “mental pain”, “tightness in the chest”, “stone on the heart” -
vital (pre-heart) melancholy ,
accompanied by a feeling of catastrophe, hopelessness, collapse.
Productive disorder. The symptom is not specific.
- during exacerbation of any mental illness
- in case of severe somatic pathology (malignant tumors)
- obsessive-phobic syndrome
- hypochondriacal syndrome
- body dysmorphomania syndrome
- !!! depressive syndrome
(syndrome-forming disorder).
Hyperthymia
is
a persistent painful increase in mood (joy, fun, delight).
— Durability
— Full of energy, initiative, interested
- Manic syndrome.
- The most acute psychoses (expressed by particularly strong exalted feelings reaching the level of ecstasy
) - may indicate the formation of “oneiric clouding of consciousness”
Euphoria -
not so much an expression of joy and happiness, but as a complacent and carefree affect.
- lack initiative
- inactive
- prone to empty talk
- delusional ideas of grandeur (with paraphrenic syndrome, in patients with progressive paralysis).
- Exogenous and somatogenic brain lesions (intoxication, hypoxia, brain tumors and extensive disintegrating extracerebral neoplasms, severe damage to hepatic and renal function, myocardial infarction, etc.)
- Paraphrenic syndrome
- Progressive paralysis
Moria
- silly, careless babbling, laughter, unproductive agitation in profoundly feeble-minded patients.
Dysphoria -
sudden attacks of anger, malice, irritation, dissatisfaction with others and with oneself.
Paroxysmal course
Capable of cruel, aggressive actions, cynical insults, crude sarcasm and bullying.
- Epilepsy (either as an independent type of seizures, or included in the structure of the aura and twilight stupefaction)
- Psychoorganic syndrome
- Explosive (excitable) psychopathy
- Alcoholism and drug addiction during abstinence
Anxiety
is
the most important human emotion, closely related to the need for security, expressed by a feeling of an impending uncertain threat, internal excitement.
Stenic emotion: accompanied by tossing, restlessness, anxiety, muscle tension
.
!!! An important signal of trouble!!!
- In the initial period of any mental illness
- Obsessive-compulsive neurosis and psychasthenia (one of the main manifestations of the disease)
- Acute delusional psychosis - a powerful, unfounded feeling of anxiety - one of the early symptoms
- Syndrome of acute sensory delirium (extremely expressed and often reaches a degree of confusion,
in which it is combined with uncertainty, misunderstanding of the situation, impaired perception of the surrounding world (derealization and depersonalization); they are looking for support and explanations, their gaze expresses surprise (
affect of bewilderment))
-
the formation
Ambivalence
is
the simultaneous existence of 2 mutually exclusive emotions (love and hatred, affection and disgust).
Causes significant suffering to patients
Disorganizes their behavior and leads to contradictory, inconsistent actions ( ambitendence ).
- Schizophrenia
- Schizoid psychopathy
- In healthy people prone to introspection ( reflection
) (in a less pronounced form)
Apathy
- absence or sharp decrease in emotions, indifference, indifference.
- Lose interest in loved ones and friends
- Indifferent to events in the world
- Indifferent to their health and appearance
Speech
: boring and monotonous, do not show any interest in the conversation, facial expressions are monotonous.
They may claim that they feel love for their parents, but when meeting with loved ones they remain indifferent, do not ask questions and silently eat the food brought to them. Lack of feelings prevents them from expressing any preference.
Negative (deficient) symptom.
- End states in schizophrenia (constantly increases, going through a number of stages that differ in the degree of severity of the emotional defect - smoothness (leveling) of emotional reactions, emotional coldness, emotional dullness
) - Damage to the frontal lobes of the brain (trauma, tumors, partial atrophy)
Differ
: a symptom
of painful mental insensibility ( anaesthesia psychica dolorosa , mournful insensibility)
is not the absence of emotions as such, but a painful feeling of one’s own immersion in egoistic experiences, the consciousness of the inability to think about anyone else, often combined with delusions of self-blame.
The phenomenon of hypoesthesia often occurs.
The vivid emotion of suffering indicates the severity of the condition and the reversible, productive nature of the disorders.
- Depressive syndrome is a typical manifestation
Syndromes of impaired will
Catatonia
– a symptom complex of mental disorders in which motor disorders predominate in the form of
akinesis
(catatonic stupor) or in the form
of hyperkinesis
(catatonic agitation).
Catatonic stupor is characterized by the presence of increased muscle tone, which develops as if from top to bottom (masticatory muscles, cervical and occipital muscles, then the muscles of the shoulders, forearms, hands and, lastly, the leg muscles). Hypertonicity may appear as stupor
or in the form of
waxy flexibility (catalepsy
).
In addition, with catatonic stupor, negativism, mutism, and passive submission
.
In accordance with the severity and predominance of certain movement disorders, several types of catatonic stupor are distinguished, which can replace each other:
a) stupor with waxy flexibility
;
b) negativistic stupor
;
c) stupor with muscle numbness
.
Catatonic excitation by an increase in motor activity, devoid of internal unity and purposefulness, with a desire to move
(in contrast to the desire for
action
in manic syndrome), against which symptoms such as
stereotypies, echo symptoms, paramimia, negativism, and passing
. May be accompanied by pathos, ecstasy, anger, rage, indifference. As a type of psychomotor agitation, it poses a danger to oneself and to others (including medical staff).
Depending on the predominance of certain disorders, several varieties are distinguished, which represent successive stages of the development of catatonic excitation:
1. confused-pathetic
excitement with exaltation, delight, pathos in behavior and speech;
2. hebephrenic-catatonic
with antics, grimacing, ridiculous antics, rude and cynical jokes, mood swings (from gaiety to anger);
3. impulsively
e excitement in the form of sudden active actions, often aggressive (they beat others, tear clothes, break objects, expose themselves, smear themselves with feces, etc.). It may be “mute” or with shouts and swearing;
4. frantic
catatonic excitement is accompanied by continuous disorderly and chaotic throwing. More often “mute”.
Stupor and excitement can appear in isolation, but they can also replace each other.
In cases where consciousness remains unclouded, catatonia is called lucid.
.
With this option, catatonia can be in the form of a monosyndrome, or it can be combined with delusions (catatonic-delusional syndrome), hallucinations (catatonic-hallucinatory syndrome), and affective (catatonic-depressive syndrome) disorders. Among the states of stupefaction, catatonia is usually accompanied by oneiric stupor ( oneiric catatonia
). Catatonic syndrome most often occurs in schizophrenia.
Violation of the dynamics of emotions
Emotional lability
- extreme mobility, instability, ease of emergence and change of emotions. They easily move from tears to laughter, from fussiness to carefree relaxation.
- Hysterical neurosis
- Hysterical psychopathy
- Syndromes of confusion (delirium, oneiroid)
One option: weakness (emotional weakness)
- not only a rapid change in mood, but also an inability to control the external manifestations of emotions, which leads to the fact that every (even insignificant) event is experienced vividly, often causing tears, which arise not only during sad experiences, but also express tenderness and delight.
- Vascular diseases of the brain (cerebral atherosclerosis)
- Personality trait (sensitivity, vulnerability)
Emotional rigidity
-
stiffness, stuckness of emotions, a tendency to experience feelings (especially emotionally unpleasant) for a long time (grudge, stubbornness, perseverance).
Speech:
thoroughness (viscosity).
General torpidity of mental processes.
- Epilepsy
- Psychopathic characters with a tendency to get stuck (paranoid, epileptoid).
“Depression cannot be cured by willpower”
“Her tentacles threatened to destroy my mind, my courage, my stomach, crush my bones, dry out my body. She gorged on me, even when it seemed like I had nothing to feed her..."
— Andrew Solomon. “Demon of the noonday. Anatomy of depression"
The word “depression” has long become something ephemeral and everyday. A serious diagnosis has become synonymous with a bad mood. “I’m depressed,” a person says, referring to being depressed due to inclement weather or being upset that a favorite team lost the World Cup.
The substitution of concepts and general misunderstanding that hover around depression give rise to endless and useless disputes between people suffering from it (in fact) and those who, with undisguised irritation, advise them to “pull themselves together.”
And now some numbers. According to the World Health Organization, depression is one of the most common mental disorders, affecting more than 300 million people of all age groups. Every year, about 800 thousand people die by suicide. Depression often causes disability. In addition, psychiatrists say that by 2020 this disease may become the leading cause of disability.
siapress issue . ru asked a local psychiatrist, author of popular books and the “Blog of Good Psychiatrists” Maxim Malyavin .
Depression and substitution of concepts
— Could you explain why depression is serious? What is hidden behind this term?
- In fact, what is actually called depression in psychiatry is very different from what the common people are accustomed to thinking of as depression. It’s one thing when a person’s mood has deteriorated for a day or two or even a week - and he says: “I’m depressed.” And it’s completely different when a sharp and significant decrease in mood is observed for three weeks or more. In this case, as a rule, the mood does not lend itself to any noticeable correction by persuasion in the spirit of “get yourself together, pull yourself together.” Precisely because it is still a disease, and not some normal reaction of the body to external changed circumstances or to an internal conflict that has arisen.
The fact is that biochemistry comes into play here. All changes affect not only the sphere of mood, but also thinking. During this period, it is noticeably more difficult for a person to think and make decisions. He sees almost no prospects, he is dissatisfied with the results of his work, whatever it may be - physical or mental. Not to mention the fact that doing all this is simply very difficult.
And here we come to the next point. During this period, not only a person’s thinking slows down, but even their motor skills. The result is a characteristic depressive triad: a significant sharp low mood, a slowdown in the pace of thinking and a decrease in the pace of physical activity. This is the classic triad for full-blown depression.
Are genes to blame for everything?
— There is a theory that depression is a hereditary disease. Tell us how it occurs and why?
“Now researchers are really more inclined to believe that genetics play a very large role in the development of depression itself, that is, genetic endowment and genetic predispositions. There are also deep-seated large-scale disturbances in biochemical processes in the brain - we are talking about the work of neurotransmitters.
In general, there is still no single coherent theory that would unite and at the same time distinguish between all types of depression. There is a lot of data, but even more needs to be collected. Nevertheless, serotonin and its influence on mood have been discovered and, accordingly, its role in the development of depression is being studied. More precisely, its lack or insufficient reaction to it. Melatonin and norepinephrine also play a role in the formation of depression.
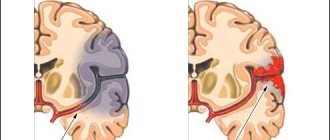
In addition, they have now begun to study brain activity during depression using so-called functional MRI. That is, this is not just a snapshot, but an observation of the functioning of the brain in dynamics with the absorption of active luminous substances. This way you can see which zones are active and which, on the contrary, are suppressed. And no less than four fairly distinct zones were found in the brain. In each case, some zone was responsible for its own special type of depression - with a predominance of apathy, with a predominance of anxiety, and so on.
— Besides heredity, what else influences the occurrence of depression?
— Sometimes depression is reactive, for example. This is a reaction to current external circumstances. This could be the loss of a loved one, dismissal from a job, the threat of loss of freedom - each has its own reason. As a rule, the way out of reactive depression is clean and good, especially if you treat it in time so that it doesn’t go too far and is not recorded in memory. As a rule, reactive depression is successfully treated. But what is genetically determined is something else. Such a person has a tendency to someday, given the sum of accumulated factors or circumstances, produce such a reaction.

Depression is quite democratic."
— Are there any statistics on who is more likely to be depressed? Residents of cities or villages, for example?
- Everyone gets sick the same way. It just turns out that the level of diagnosis and the number of those found are different. Where there are more specialists, they find more. Where there are no specialists, no one “suffers from depression” at all.
— Are women and men equally prone to depression? They usually say that the weaker sex is more vulnerable.
— It is generally accepted that women, due to their greater emotionality, seem to have a higher percentage of depression, but this is actually not such a noticeable difference. Depression is quite democratic - gender, wealth and social status are not important to it.
— There is a common stereotype that wealthy people or dreamy youth, for example, simply have nothing to do - so they indulge in the blues.
- It's really worth distinguishing. There is, for example, the once fashionable word “spleen,” but there is something more difficult and caused not only and not so much by external circumstances, but precisely by those things that happen inside.
There is, for example, postpartum depression - when a woman feels so bad that she is ready to take extreme measures with her child, because she sees no prospects in life either for herself or for him.
But there is something else and quite understandable psychologically. A woman understands that over the next few years a fairly large burden will fall on her shoulders, and some begin to feel complex that after giving birth they have become less attractive, and so on. This condition, explained and caused by external factors, is called baby blues. This is not postpartum depression.
From champagne to antidepressants
— How to treat depression? How are the old methods different from the new?
— Depression has been treated for centuries. It’s just that in each era the approach to its treatment was at a level equal to the idea of what it is and what can be done with it due to technical capabilities.
The 19th century psychiatrist Krafft-Ebing wrote that it would be a good idea to give champagne to patients with depression. A little later, there were attempts to treat depression with cannabis, and then cocaine. There was a time when doctors tried to involve amphetamines and their derivatives in this case.
It turns out that only in the 50s the bread of psychiatry was discovered - aminazine. One of the substances used to treat tuberculosis patients caused them an unnatural mood lift. Moreover, this applied to patients whose mood was initially reduced. Thus, observations emerged that made it possible to discover the first antidepressants. Well, then a whole galaxy of such drugs appeared.
Myths and facts about antidepressants
— There is an opinion that you can get hooked on antidepressants. Many people advise on forums not to take pills and boast that they have given up medications. What do you have to say about this?
— Antidepressants have criteria by which they were created, as well as distinctive properties inherent in them.
An antidepressant only acts on painfully depressed mood! If a person has a normal mood, an antidepressant will not increase it in any way - it is not a stimulant.
The second point is that it is almost impossible to get hooked on antidepressants. They do not give you the feeling of a buzz, which, by the way, is the same with tranquilizers (Valium, Diazepam, Seduxen and others). But they, in fact, had other tasks. Now doctors are slowly trying to move away from the use of tranquilizers. Other drugs are being developed.
Antidepressants do not have such an effect that would make you want to take them more and more. On the contrary, when a person starts taking antidepressants, most often nothing happens during the first week and a half to two weeks. He just doesn't feel anything. In addition, sometimes there are some side effects that can be unpleasant: dry mouth, nausea, constipation. This usually occurs while taking fairly strong drugs. However, here’s the problem: nothing happens to your mood!
The fact is that the antidepressant must be involved in biochemical processes. The amount of neurotransmitters must accumulate. And only after some time will this whole colossus, this whole hefty aircraft carrier called “mood” change course!
At the same time, when they say that they will assign them to you, they say, and you will not get off them, people confuse cause and effect. Depression is not a cold; it will not go away in 10 days. To establish biochemistry, set the normal course and make a foundation for the future, a minimum course of antidepressants of 6-8 months is required.
— Does it take six months to actually achieve a lasting effect?
- Yes, persistent and distant - for the future. It happens that a person has taken pills for a month or a month and a half, his mood has developed, and he feels good. He says, that’s it - I’m not sick anymore, why would I drink them? He throws them away, but it’s not over yet! These are external signs and subjective sensations. Besides, it also costs money. And they also like to say here that it’s all chemistry.
At this moment, the most common mistake occurs: depression has not ended, but the person has already stopped taking antidepressants. Accordingly, about three or four weeks pass, and everything returns.
However, a person cannot regard this correctly - as a disease that he has not cured. He believes that he was hooked on pills, and this is not a relapse of depression, but a withdrawal syndrome.
— Is it true that an important part of treating depression is also direct work with a psychotherapist, and not just taking medications?
- This is not always necessary. In some cases, a person has enough of his own common sense to understand what he needs. In addition, it is not always possible to connect a psychotherapist right away. Let’s say that a person’s situation is completely bad - it’s not just that he was going to do something to himself, but mentally he did everything a long time ago, and managed to develop a plan. The only thing that can hinder him is the lack of strength to pull himself together and do what he has planned, or the remnants of awareness of his duty to his family and friends. He is in such a bad mood that he is in physical pain. There is such an expression for clinically developed depression - “vital melancholy”. It’s a feeling as if your chest is being torn from the inside, torn apart by claws, a knife. Physically it hurts. Imagine: a psychotherapist comes to the patient and says: “Let’s talk about this.” “I should have shot him, the dog!” - the patient thinks at this moment.
A psychotherapist usually (not only for depression, but also for other acute severe conditions in psychiatry) appears in the patient’s field of vision only when the severity has subsided and when the patient is able to hear what is being said to him.
But if we are talking about the fact that depression occurs, but it is not very pronounced and, let’s say, what is required from a psychotherapist is not so much techniques that could help you look at life differently, but simply participation and basic medical education, then a specialist is needed.
When to see a doctor
— How do you know when to contact a specialist? What should you be wary of?
- First of all, this is the duration of the pronounced decrease in mood. When it’s really not just so-so, but bad. Moreover, not a day or two, but about three weeks. This is conditional. Times may vary. At this moment, nothing makes you happy, sex is not relaxing - and there’s no time for it at all. Sometimes friends say, just drink and it will be better. A depressed person should not be offered a drink! Alcohol enhances the state in which a person is. Depression will get worse, nothing good will come from alcohol.
Let's get back to the symptoms. There is one more symptom characteristic of major clinical depression. If in the morning the mood seems to be tolerable, but in the evening melancholy and hopelessness sets in and gets worse, then this is also a sign.
But if everything is bad in the morning, but in the evening, on the contrary, it becomes a little easier - this is more likely a sign not of depression, but of subdepression and the accompanying attenuation and nervous exhaustion.
In addition, if all these conditions are accompanied by loss of appetite and insomnia, then it is advisable not to hesitate and consult a specialist.
What to tell people if you are depressed?
- There is such a moment. People with a real diagnosis often hear phrases like “get yourself together, pull yourself together,” “I did it, and don’t be a wuss,” and so on. What should they answer to their advisers? Is it possible to cure depression with willpower alone?
- No, depression cannot be cured by willpower. With the help of willpower you can only try to survive it. Yes, it happened before that we did without medicine and so on. Depression played out its time, and then there even seemed to be an improvement. But the moment when she wins back could drag on for a year or more! What modern person is ready to allow himself to fall out of active life for a year? And it’s very painful for yourself. It seems simple: one! - and you do nothing. But you don't do anything because you feel so bad that you simply can't do anything. And this is if real noticeable suicidal tendencies and moods are not involved...
You see, it's a thankless task to try to tell someone how to respond to people who haven't experienced it or haven't seen people with depression in huge numbers. It's like explaining to a man how to give birth.
Reference : Depression is a complex of mental disorders associated primarily with the emotional sphere. The disorder is characterized by various disturbances in which people experience sadness, anxiety, guilt, anhedonia (loss of the ability to experience pleasure), or apathy (lack of both negative and positive emotions). Depression is characterized by certain disturbances in the area of thinking. When people are depressed, they have difficulty making decisions. They have dark thoughts about themselves, about the world around them, about people. Depression has physiological manifestations such as disturbances in sleep, bowel function, and sexual needs. In patients with depression, their overall energy tone is disturbed and they feel fatigued. With somatized depression, a person experiences unpleasant sensations in the body.
Drawings: Nadya Makarenko