Humans have a remarkable ability to control their emotions. They laugh when they are happy, cry when they are in pain (physical or emotional), and get angry when they are upset. We humans are gifted with a variety of emotions and as we get older, we develop the ability to express them at the appropriate moment. Almost everyone can experience a fit of laughter, sudden irritability, or a fit of crying and sadness. These things release our repressed emotions - this is normal. At times, however, for some, emotions are out of control and understanding. An emotionally labile person may laugh at a funeral, or may begin to cry at a joke, or become irritated and angry for no apparent reason. These emotions, as a rule, are extremely violent. Emotional lability is a disorder that is characterized by involuntary emotional manifestations of mood in an excessively severe form. Individuals suffering from this condition are prone to fits of uncontrollable laughter, outbursts of anger and bouts of crying. These emotions have nothing to do with a person’s emotional state. Emotional lability occurs in people who suffer from certain diseases, head trauma, or after a stroke. It can occur due to two main reasons: physical damage to the brain or emotional distress. In cases of physical damage, the brain and nervous system are damaged due to aging or injury. If a person has faced severe emotional shock, experienced tragic events, such as the loss of family, relationships, work, etc. - this may also cause lability. The following are some possible medical causes of emotional lability: brain injury, attention deficit hyperactivity disorder, Alzheimer's disease, amyotrophic lateral sclerosis, brain tumor, Creutzfeldt-Jakob disease, Cushing's disease, dementia, depression, head injury, HIV syndrome, Huntington's disease , lead poisoning, previous encephalitis, postpartum depression, pseudobulbar palsy, postpartum psychosis, mental illness, motor neuron disease, multiple sclerosis, neurosyphilis, hydrocephalus, stroke, Usher syndrome. Emotional lability is not a permanent condition. The important point here is the triggering moment, those situations that can cause outbursts of uncontrollable emotions. Some of these triggers include: fatigue, certain stimuli (crowds, high expectations, noise), anxiety, insulin imbalance, thyroid hormone imbalance, menstruation/premenstrual syndrome/menopause, high blood pressure. Now that you know the cause of these emotional reactions, and what things can trigger them, it's time for the next step, and that's part of the treatment. Treatments typically focus on teaching the person how to manage this sudden surge through cognitive behavioral therapy, counseling, support groups, yoga, breathing exercises, relaxation techniques, stretching, etc. Before starting any treatment, it is advisable to visit a doctor. He will be able to better determine the cause of the problem and prescribe effective treatment and medications. Certain rules should be followed: - People around the patient can be the main irritants for the development of an attack. Therefore, not only the patient, but also the people around him should be educated. This will help the patient to be free from additional tension and stress. - Take a break, take short breaks, go for a walk, or sit with a cup of tea, this will help you relax, reduce internal tension and help in the fight against anxiety. - Try to ignore, not pay attention to the behavior of such a person, which will help him relax in the future. Treat the behavior—whether laughing, angry, crying—as insignificant and continue the conversation until the attack passes. - Avoid stressful factors, exclude certain topics that can cause stress in the patient, try to change the topic and distract the person. Avoid noisy crowded places and eliminate loud sounds. Receiving a psychotherapeutic consultation by a patient will help a person cope with his deep-seated problems and eliminate the cause of the problems. The doctor can give the patient enough instructions on how to deal with difficult situations. In some cases, medications may be prescribed. Early detection of symptoms of emotional lability along with proper treatment will help prevent further progression of this condition and preserve the patient’s relationships with people close to him.
The term “lability” means instability, mobility, variability of various phenomena and processes in the body (pulse, body temperature, physiological state, psyche).
Autonomic lability is the unstable functioning of the autonomic (autonomic) nervous system.
Increased sensitivity and reactivity of the autonomic nervous system manifests itself with minimal stress.
Anatomical and physiological implications
The autonomic nervous system is part of the body's nervous system. Its functions include control and regulation of the work of internal organs (intestines, stomach, heart, etc.), lymphatic, circulatory systems, and glands of the body.
This system also regulates the process of sweating, heart rate, thermoregulation, and blood pressure. It is also responsible for a person’s reaction in stressful situations, for the ability to fully relax physically during rest, for the digestion and assimilation of food consumed. The functioning of the autonomic nervous system is beyond human control.
The autonomic nervous system consists of two divisions - sympathetic and parasympathetic. The parasympathetic nervous system regulates the functioning of the endocrine system, the digestive tract, is responsible for metabolism and lowering blood pressure.
The sympathetic nervous system is active in stressful situations. It is responsible for supplying muscles with oxygen, rapid heartbeat, and breathing.
In a normal state, there is an adequate response of the autonomic system to external stimuli (stress, temperature, sounds). With the syndrome of increased lability of the autonomic nervous system, an individual may experience inadequate reactions to common stress factors: increased sweating at low temperatures, increased blood pressure with minor stress.
Reflexes of the autonomic system ensure an adequate response of the body to stress, and a person’s understanding of the presence of anomalies in his condition or sensations.
Autonomic lability is not an idiopathic disease. Often it is a sign of vegetative-vascular dystonia. This disorder is present in approximately 80% of the population, in adults and children.
At this stage of selection, the main criterion for assessing the prospects of a young athlete is whether he has the ability to effectively improve sports. After 2-3 years of initial training and long before reaching the optimal age limit in a particular sport, it is still impossible to give an accurate conclusion about whether a young athlete has the inclinations and abilities that allow him to hope to achieve international-level results. However, it is necessary to identify the feasibility of further sports improvement and determine its directions, and correctly orient the athlete’s further training. These problems can be solved only on the basis of a comprehensive analysis, which should take into account the morphological, functional and mental characteristics of young athletes, their adaptive capabilities, reaction to training and competitive loads, ability to master and improve new movements, etc.
Sports results at this stage of selection cannot be a criterion for prospects. Experience shows that athletes with relatively low results at the beginning of the preliminary basic training stage are among the strongest at the end of it and continue to progress in the future. At the same time, winners and prize-winners of children's and adolescent competitions very rarely (less than 5% of cases in different sports) achieve sporting success at the stage of maximum realization of individual capabilities. This is convincingly evidenced by many years of experience in training high-class athletes in various countries around the world.
Already at the beginning of the second stage of long-term training, the need arises to determine the correspondence of the body structure of young athletes to the morphological characteristics of high-class masters. Morphological features are among the most important that must be taken into account when determining the prospects of an athlete at this stage of selection. Morphological differences between representatives of different sports are a consequence of intensive selection, since the structural features of the body give the athlete purely mechanical or biomechanical advantages in competitions in various sports. Although the human constitution experiences some changes at certain age periods, in general it is more or less constant and is largely determined by hereditary factors.
It should be noted that there is no single approach to determining the human constitution. This applies both to the definition of the very concept of “human constitution” and to the diagnosis and characteristics of constitutional types. The most common approaches to determining the human constitution are based on morphological criteria - the degree of muscle development and fat deposition, height and body weight, skeletal features, etc. With this approach, most experts tend to use the term “somatotype” to characterize the constitution.
Morphofunctional examinations can be supplemented by biological studies of muscle tissue that bear the main load in a given sport. It is advisable to analyze muscle tissue once at the second stage of selection. However, it should be taken into account that the percentage of muscle fibers of various types is closely related to the functional capabilities of the athlete. In particular, an athlete’s high alactic capacity, good motor response, high results in speed-strength tests (for example, standing jump) and others are a guarantee of the presence of an increased number of muscle fibers. And, on the contrary, a slow reaction, high capabilities of the oxygen transport system and oxygen utilization system indicate the predominance of MS fibers in the athlete’s muscles (Platonov, 1991; De Vries, Houch, 1994).
Of great importance for the rational selection and orientation of young athletes at this stage is the analysis of the properties of their nervous system - the strength of the processes of excitation and inhibition, their balance and mobility. The strength of nervous processes characterizes the ability of nerve cells to tolerate strong excitation and strong inhibition, which allows them to adequately respond to irritation. Balance presupposes a certain relationship between the processes of excitation and inhibition, and their mobility is expressed in the ability of the nervous system to quickly alternate these processes. Different individuals may have a wide variety of combinations of properties of the nervous system, which largely determine not only the psychological, but also the functional capabilities of athletes (Volkov, Filin, 1983; Arnot, Gaines, 1992; Wilmore, Costill, 2004). In particular, such as the effectiveness of muscle-motor differentiation, the ability to adequately assess the functional state, perceive emerging situations, make and implement creative decisions, etc. (Rodionov, 1973; Weinberg, Gould, 2001).
When considering the prospects of an athlete based on morphological type indicators, one should give not only a holistic assessment (based on the same indicators as at the previous stage of selection), but also guide the athlete towards specialization in a particular distance or discipline. Thus, in swimming, tall teenagers with long limbs and great strength capabilities of the muscles of the shoulder girdle can be targeted for specialization in sprinting; for long distances - children with good buoyancy and streamlining of the body, high capabilities of the oxygen transport system, good mobility in the ankle joints (Bulatova, 1996).
Adolescents with above-average height and greater strength capabilities of the leg muscles should be targeted for specialization in short-distance running; in long-distance running - adolescents with a small mass and height index and high oxygen transport system capabilities. Body length is not significant here (Volkov, 1989; Tittel, Wutscherk, 1991; Wilmore, 1992).
After a fundamental decision on the advisability of further continuing classes at the stage of preliminary basic training, the most promising direction for improving the young athlete, which meets his natural inclinations, should be identified. It is very important here to clearly understand that, according to survey data, young athletes can be divided into different groups depending on their predisposition to achieve high sports results not only in various sports, but also in various types of competitions of the same sport. Athletes specializing in swimming, for example, can be divided into five relatively independent groups - based on a wide range of indicators that reflect the predisposition of young athletes to sprint or stayer work.
The first group is athletes with pronounced sprinting abilities (sprinters).
The second group consists of athletes with mixed abilities, with a predominant predisposition to sprint work (mixed athletes with a predisposition to sprint work).
The third group consists of athletes with mixed abilities with a relatively uniform level of their development.
The fourth group is athletes with mixed abilities, with a predominant predisposition to stayer work (mixed athletes with a predisposition to stayer work).
The fifth group is athletes with pronounced staying abilities (stayers) (Bulatova, 1996).
These groups are unevenly represented in the general population. Pure sprinter or stayer types are relatively rare; most athletes belong to various intermediate types (Fig. 1.5).
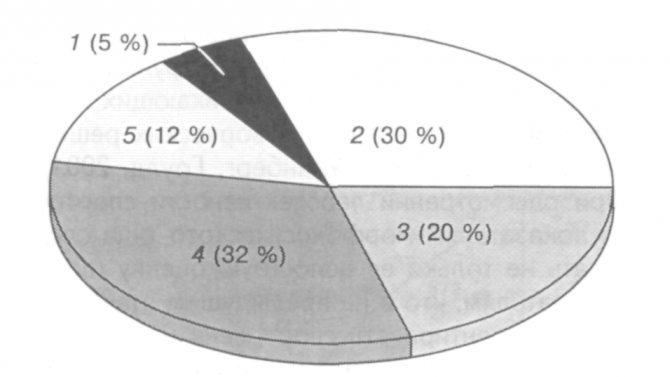
Rice. 1.5 Representation of athletes of various groups in the general population: 1 - sprinters; 2 - mixed doubles with a predisposition to sprint work; 3 - mixed teams with mixed abilities; 4 - mixed teams with a predisposition to stayer work; 5 - stayers (Bulatova, 1996)
Swimmers included in each of the five groups differ significantly from each other in basic anthropometric characteristics, the capabilities of the energy supply system, psychophysiological characteristics, and the level of development of special motor qualities.
Athletes from the first group (sprinters) are distinguished by large values of height, body weight, girth dimensions, length of the upper and lower extremities (Table 1.8). They have high anaerobic power and functional mobility and are superior to athletes from other groups in terms of alactic and lactate work capacity, maximum oxygen debt, coefficient of increase in oxygen consumption, time to reach maximum oxygen consumption (Table 1.9).
Indicators of psychophysiological characteristics of these swimmers indicate high lability of their nervous system, reactivity (Table 1.10), and special motor tests indicate a high level of absolute swimming speed and explosive strength, low gliding length and aerobic endurance (Table 1.11).
Athletes from the third group (mixed athletes with mixed abilities) are distinguished by average anthropometric data, high values of maximum oxygen consumption, oxygen debt, long time of holding critical load power, significant oxygen pulse and maximum critical load power (see Table 1.9). In special motor tests, swimmers from the third group showed a lower level of absolute swimming speed and jumping height than athletes from the first group, but they significantly differed in the best time to cover the distance of 2000 freestyle and a longer glide length (see Table 1.11).
Swimmers from the fifth group are distinguished by a high level of power and stability of the aerobic energy supply system, assessed by the indicators of maximum oxygen consumption, maximum critical load power, maximum oxygen pulse, time of maintaining critical load power (see Table 1.9). At the same time, representatives of this group have low rates of motor reaction, low tempo of movements, and low lability of the nervous system (see Table 1.10). In special motor tests, these athletes have a long glide length and a high level of aerobic endurance as a result of swimming a distance of 2000 m, mediocre results in absolute swimming speed and jumping height (see Table 1.11). In general, the results of these studies provide quite convincing evidence of the high information content of the used set of indicators. The above approach is highly effective for orienting young athletes at the stage of preliminary basic preparation for sprint or stayer work. When specifically addressing this issue, differentiated models can be used to classify a young athlete into one group or another (Fig. 1.6, 1.7). It is possible with fairly high reliability to orient the training system of young athletes of each of the five groups towards achievements in swimming at distances of various lengths (Table 12).
Table 1.8
Basic morphological indicators of young swimmers aged 11 - 13 years with sprinting, staying and mixed abilities (Bulatova, 1996)
| Index | Group of athletes | ||||
| First | Second | Third | Fourth | Fifth | |
| Height, cm | 164,44±0,20 | 157,14±0,11 | 152,0±0,20 | 150,0±0,31 | 149,12±0,20 |
| Body weight, kg | 52,10±0,51 | 46,21±0,01 | 42,20±0,62 | 41,22±0,02 | 40,82+0,42 |
| Arm length, cm | 76,51±1,67 | 73,42±0,20 | 70,0±3,0 | 67,32±0,92 | 65,10±1,05 |
| Leg length, cm | 90,30±2,52 | 86,20±1,55 | 82,10±1,44 | 79,10±0,84 | 76,20±1,21 |
| Brush length, cm | 17,08±0,53 | 16,20±0,52 | 15,10±1,0 | 14,26±0,51 | 13,42±0,38 |
| Shoulder circumference, cm | 26,31±1,37 | 25,23±0,52 | 23,14±2,76 | 21,34±0,53 | 20,24±0,32 |
| Forearm circumference, cm | 24,82±0,92 | 23,42±0,63 | 22,14±0,97 | 20,64±0,82 | 19,83±0,43 |
| Thigh circumference, cm | 51,0±2,01 | 47,53±0,83 | 45,0±0,95 | 40,0±0,89 | 38,0±1,23 |
| Shin girth, cm | 35,42±0,05 | 33,20±0,51 | 31,12±1,58 | 29,32±0,22 | 27,0+1,02 |
| Pelvic circumference, cm | 88,52±2,41 | 80,23±0,51 | 79,52±0,52 | 75,32±0,88 | 71,21±1,25 |
| Shoulder width, cm | 35,27±1,02 | 33,34±0,52 | 32,32±0,94 | 30,23±1,05 | 28,12±0,89 |
| Pelvic width, cm | 25,0±0,52 | 23,42±0,51 | 22,42±0,86 | 20,34±1,08 | 19,14±0,52 |
| Brush width, cm | 8,83±0,31 | 7,93±0,32 | 7,21±0,52 | 6,83±0,52 | 6,43±0,25 |
Table 1.9.
Characteristics of the capabilities of the energy supply system for swimmers with sprint, stayer and mixed abilities when performing loads on a diagnostic stand (Bulatova, 1996)
| Index | Group of female athletes | ||||
| First | Second | Third | Fourth | Fifth | |
| Power of functional systems | |||||
| Alactate work power, W/kg | 9,32+0,06 | 8,90±0,02 | 8,02±0,09 | 6,91±0,09 | 6,51±0,10 |
| Lactate work power, W/kg | 6,73±0,09 | 6,36±0,01 | 5,67±0,07 | 4,83±0,06 | 4,62±0,07 |
| Oxygen debt, ml/kg | 108,0±0,31 | 97,83±0,82 | 81,3±1,65 | 63,62±0,40 | 59,31±1,12 |
| Maximum oxygen consumption, ml/kg | 48,72±0,71 | 51,31±0,73 | 62,31±0,97 | 70,62±0,42 | 78,84±0,97 |
| Critical load power, W/kg | 2,92+0,13 | 3,01±0,82 | 3,42±0,14 | 4,41±0,06 | 4,82±0,06 |
| Oxygen pulse, ml/beat.1 | 10,23±0,21 | 11,6±0,36 | 13,73±0,25 | 15,42±0,37 | 18,73±0,25 |
| Functional mobility | |||||
| Coefficient of increase in oxygen consumption, conventional units - | 11,41 ±0,34 | 8,60±0,93 | 7,75±0,24 | 5,82±0,54 | 4,72±0,23 |
| t50 output to VO2max, s | 27,10±0,13 | 31,38+0,72 | 41,30±0,13 | 48,51±0,54 | 58,02±2,31 |
| Stability of functional systems | |||||
| Time to maintain critical operating power, min | 178,02±0,23 | 201,92±0,30 | 260,44±0,71 | 310,0±0,20 | 380,02±3,02 |
Table 1.10
Psychophysiological characteristics of swimmers with sprinting, staying and mixed abilities (Bulatova, 1996)
| Index | Group of female athletes | ||||
| First | Second | Third | Fourth | Fifth | |
| Motor reaction time, ms | 154,02±0,02 | 162,0±0,02 | 188,03±0,02 | 215,02±0,02 | 234,03±0,03 |
| Number of movements in 10 s | 84,0±1,0 | 75,0±1,0 | 62,0±1,0 | 58,0±1,0 | 52,0±1,0 |
| Strength of the nervous system (by the nature of the performance curve, tapping test) | Strong, weak | Strong, weak | Medium-strong, weak, medium-weak | Medium-strong weak, medium-weak | Strong, weak |
| Lability of the nervous system (tapping test) | High, above average | High, above average | Above average, average, below average | Above average, average, below average | Average, below average |
Table 1.11
Level of development of special motor qualities of swimmers with sprinting, staying and mixed abilities (Bulatova, 1996)
| Index | Group of female athletes | ||||
| First | Second | Third | Fourth | Fifth | |
| Absolute swimming speed, ms | 1,62±0,01 | 1,55±0,02 | 1,46±0,01 | 1,35±0,01 | 1,31±0,01 |
| Result of swimming 2000m freestyle, s | 2630,81±30,53 | 2320,50±114,02 | 2024,31±30,30 | 1770,12±12,11 | 1698,03±47,11 |
| Sliding length, m | 6,60±0,11 | 7,54±0,72 | 8,50±0,13 | 9,72+0,23 | 11,38±0,42 |
| Jumping height, cm | 52,0±0,10 | 49,0±0,20 | 40,00+0,0 | 33,50+0,30 | 33,0±0,10 |
Rice. 1.6 Structure of functional readiness of young sprint swimmers (a) and stayers (b) (as a percentage in relation to the indicators of the general mixed model - circle): 1 - time of holding the critical load power; 2 - maximum oxygen consumption; 3 - critical load power; 4 — alactic power of work; 5 — lactate work capacity; 6 — motor reaction time; 7 - absolute swimming speed; 8 — jumping height.
Rice. 1.7 Morphological characteristics of young sprint swimmers (a) and stayers (b) (as a percentage in relation to the indicators of the general mixed model - circle): 1 - height; 2 - body weight; 3 - shoulder circumference; 4 - forearm circumference; 5 - pelvic girth; 6 — brush width; 7 — shoulder width; 8 — pelvis width; 9 — arm length; 10 — brush length; 11 — leg length; 12 - thigh circumference
It has been experimentally established that the use of differentiated training programs for young athletes, built in accordance with the individual predisposition of swimmers to achieve achievements at distances of various lengths, is an effective factor in increasing the effectiveness of training at the stage of preliminary basic training in the system of long-term sports improvement.
A similar approach can be successfully implemented not only in cyclic sports, for example in track and field running or speed skating, but also in sports games and martial arts, making it possible to identify in advance the strongest sides of an athlete, correctly determine his playing role, the directions of technical, tactical and physical improvement, optimal model of competitive activity.
A promising genetic marker of an athlete's functional capabilities for a number of sports is hand dominance. Left-handed athletes, compared to right-handed ones, have a higher speed of simple motor reaction, which ensures the success of simple actions, they are characterized by a high level of anxiety, an unbalanced type of nervous system, and a predominance of object-based thinking. At the same time, they are inferior to right-handed people in the speed of decision-making in difficult situations and in the ability for abstract logical thinking. These characteristics of left-handed athletes, determined genetically by 40-50%, determine their success in activities that require exceptional reaction and the execution of relatively simple movements at high speed (Sologub, Taymazov, 2000). This is most clearly manifested in fencing: among the champions of major international competitions, the representation of left-handed athletes is 10 times higher than the average population data and amounts to about 50%. It is these athletes who are distinguished by their simplicity and exceptionally high speed of action (Nikolskaya, 1993).
In other sports, left-handed athletes are distinguished by a wide variety of technical and tactical actions. In boxing they can work in both right- and left-handed stances, in figure skating they perform rotations both to the right and to the left, in volleyball and handball they successfully use hits and throws with both right and left hands. All this, naturally, should be taken into account when orienting the process of training such athletes at all stages of their long-term improvement, both in relation to the construction of the process of technical and tactical improvement, and the selection of optimal models of competitive activity.
Table 1.12
Predisposition of young swimmers from various groups to achieve achievements at distances of various lengths
| Groups of swimmers | Predisposition to achieve at distances, m | ||
| High | Average | Low | |
| Sprinters | 50 | 200 | 800 and 1500 |
| Mixed athletes with a predisposition to sprint work | 100 and 200 | 400 | 1500 |
| Mixed athletes with mixed abilities | 200 and 400 | 100, 800 and 1500 | — |
| Mixed athletes with a predisposition to stayer work | 800 | 200 | 50 |
| Stayers | 1500 | 400 | 100 and 50 |
Reasons for failure
Lability of the autonomic nervous system can develop gradually and occur suddenly. This condition often remains undiagnosed, since patients do not attach importance to the manifestations, considering them the result of stressful situations and fatigue. Patients may also be considered hypochondriacs.
The causes of autonomic lability can be varied:
- stress factors;
- adverse effects of the external environment;
- infectious diseases;
- intoxication;
- surgical intervention;
- traumatic brain and other injuries;
- change of climate and time zones;
- pregnancy;
- menopause;
- psychological trauma, including childhood trauma;
- lack of vitamins (especially vitamins B1, B3, B6 and B12 and vitamin E).
Peculiarities
Not so long ago, autonomic lability was considered a disease that was diagnosed primarily in adults. However, in recent decades the situation has changed dramatically, and this diagnosis is given even to children.
In children
Experts are unanimous in their opinion as to why autonomic lability syndrome is increasingly being discovered in children. The main reason is too much workload: first - school, then - all kinds of sections and clubs. Everything is aggravated by the harmful effects of modern gadgets. However, this diagnosis is also made to very young children due to complications of pregnancy and childbirth.
The peculiarity of the course of the disease in children is due to the fact that at each age its manifestations change.
At the age of 0-2 years:
- problem with the gastrointestinal tract,
- body weight deficiency,
- skin problems,
- severe allergic reactions,
- bad dream.
2-4 years:
- weather sensitivity,
- weakening of the immune system,
- poor appetite
- high impressionability, phobias, closedness, pathological attachment to one of the relatives.
5-10 years:
- nightmares,
- frequent tantrums,
- pallor, excessive thinness,
- rapid fatigue
- lipothymia (conditions close to fainting),
- headache.

In adolescence, this type of lability turns into vegetative-vascular dystonia.
During therapy, non-drug methods are most often chosen: exercise therapy, massage, physiotherapy and herbal medicine, breathing exercises.
In adults
In adults, lability of the autonomic nervous system is diagnosed primarily in the period from 20 to 30 years. Leading an unhealthy lifestyle makes itself felt: lack of routine, unhealthy diet, inadequate sleep.
Women are diagnosed with this condition almost 3 times more often than men. This is explained by the fact that during certain periods of life (pregnancy, after childbirth, menopause) they experience hormonal imbalances, which lead to disturbances in the functioning of the ANS.
However, there is an opinion that these data are inaccurate, and men are diagnosed with this less often, not because they are not characterized by vegetative lability. Firstly, with such symptoms they do not seek medical help. Secondly, they use their own methods to combat them (for example, alcohol).
Wide range of manifestations
Manifestations of autonomic lability are associated with all areas that are controlled by the autonomic nervous system; symptoms of the condition can be varied:
- fainting and dizziness;
- increased fatigue (due to lack of adequate adjustment of heart rate relative to stress);
- increased or decreased sweating;
- headache;
- disturbances in the digestive tract, which lead to constipation, diarrhea, bloating, loss of appetite;
- difficulty urinating;
- problems in the sexual sphere (lack of erection, vaginal dryness, nonorgasmia);
- visual impairment (increased sensitivity to light, blurred vision);
- poor tolerance to cold and heat;
- sleep disorders;
- tremor;
- rapid heartbeat, lability of blood pressure;
- apathy, lethargy, weakness, constant mild malaise;
- increased irritability;
- decreased concentration;
- sudden mood swings;
- speech disorders;
- unreasonable fears, anxiety and neurotic phobias;
- pain in joints and muscles;
- dry skin;
- numbness in various parts of the body.
Blood pressure lability
Another expression found in medicine. It is characterized by a permanent or temporary manifestation of either an increase or decrease in blood pressure. Such jumps can manifest themselves through headaches in the back of the head, “floaters” and double vision, sleep disturbance, decreased attention and memory, numbness of the limbs, as causeless excitability and irritability. You need to pay attention to these symptoms and also try to determine the cause of their occurrence. You need to measure your blood pressure twice a day for about two weeks and try to change your lifestyle - diet, sleep patterns, spend more time in the fresh air, pay attention to sports, reduce physical and psycho-emotional stress.
Examination and diagnosis
To make a diagnosis, a comprehensive examination is necessary, since the symptoms of autonomic lability are similar to those of other diseases. It is necessary to exclude mental illnesses, neuropsychiatric disorders, and also in the case of physiological manifestations, to exclude organic pathologies.
After excluding other diseases, the likelihood of disorders in the autonomic nervous system is considered. Often, collecting an anamnesis, interviewing the patient, and a superficial examination is sufficient.
A neurologist should pay attention to constriction or dilation of the pupils, increased sweating, or excessive dryness of the skin, pallor, or hyperemia of the skin. To assess the work of the autonomic system, the work of skin, somatovegetative, and sweat reflexes is analyzed.
Also, to assess the degree of violations, tests are prescribed for the biochemical composition of urine and blood.
What it is

Autonomic lability is a malfunction in the activity of the autonomic nervous system (hereinafter abbreviated as ANS). Its main purpose is to adapt the functioning of the body to environmental changes, ensuring homeostasis. An example is sweating as a natural way to cool the body through evaporation. However, the ANS determines not only the physiological state of a person, but also takes part in his behavioral aspects, and therefore in his mental activity.
If the ANS is functioning normally, the person feels good in all respects. But as soon as it malfunctions, inexplicable things begin to happen: my head hurts, my hands tremble, sweat appears on my forehead. And in parallel with this, irritation increases for no apparent reason, you want to cry, lie down and do nothing. It is this borderline state, when both the body and the psyche fail, that is vegetative lability.
Many experts insist that it is not an independent disease, since it includes symptoms of various abnormalities in the functioning of the ANS:
- somatoform-vegetative dysfunction of the nervous system (vegetative-vascular dystonia),
- autonomic disorder,
- vegetative neurosis,
- autonomic-vascular type of hypothalamic crisis,
- psychovegetative syndrome, etc.
In this regard, sometimes autonomic lability is spoken of not as a separate disease, but as a complex syndrome.
An integrated approach to treatment
When treating vegetative lability, methods without the use of pharmacological drugs predominate.
To bring the functioning of the nervous system back to normal, it is recommended:
- adhere to normal operating hours;
- have proper sleep and rest;
- follow proper nutrition;
- lead a healthy lifestyle;
- exercise;
- reduce physical activity;
- spend time outdoors, take walks;
- avoid stress factors;
- use decoctions of mint, valerian, lemon balm.
Drug treatment consists of the use of drugs that calm the nervous system, as well as symptomatic treatment of organs and systems whose functioning has been disrupted due to the disease.
Treatment
Medication
For vegetative lability, in some cases medications are prescribed:
- sleeping pills,
- painkillers,
- sedatives (Atarax),
- vitamin complexes,
- tranquilizers (Adaptol),
- to normalize vegetative-vascular disorders in particular cases, Corvalol, Valocordin, Glycine can also be prescribed.
The drug course is selected exclusively by a neurologist, taking into account the individual characteristics of the patient.
Non-drug
However, a non-drug course of treatment is usually prescribed, which consists of patients following a number of recommendations:
- adhere to the basic principles of a healthy lifestyle,
- normalize the daily routine,
- get enough sleep,
- eat well,
- provide physical activity,
- breathe more fresh air,
- avoid stress,
- drink infusions and take baths with herbs: peppermint, valerian, lemon balm.
All these recommendations provide a complete answer to the question of how to treat this disease yourself, without the involvement of specialists. But doctors warn about the dangers of this approach to eliminating the main symptoms of vegetative lability, because they may be signs of another disease that requires completely different therapeutic methods.

Of considerable importance in treatment is the help of a psychologist who:
- helps to identify the main provoking and traumatic factor of the ANS (hypnosis may be used),
- teaches how to cope with phobias, fears, stress (through affirmations, auto-trainings),
- teaches psychological techniques for quickly eliminating vegetative symptoms.
Exercise therapy, therapeutic massage, reflexology, breathing practices, lithotherapy, balneotherapy, and electrophoresis can also be prescribed. Their task is relaxation, activation of blood and lymph flow, relieving muscle spasms and stress tension.
Therapeutic diet
Experts advise increasing the amount of foods rich in certain vitamins and minerals in your diet, which are important for the normal functioning of the ANS:
- Phosphorus: processed cheese, fish, feta cheese, shrimp, cottage cheese.
- Iron: nuts, liver, spinach, lentils, peas, buckwheat.
- Calcium: nuts, garlic, cottage cheese, sour cream.
- Magnesium: nuts, buckwheat, kelp, barley, oatmeal.
- Potassium: dried apricots, beans, kelp, peas, prunes, raisins.
- Iodine: feijoa, fish, squid, shrimp, kelp.
- Vitamins: fresh fruits, vegetables, berries, grains, fish oil.
- Fiber: cereals, bran, seeds, figs.
- Lecithin: legumes, nuts, eggs, seeds, olives, citrus fruits, avocados, sprouted grains.
Proper nutrition with such a diagnosis is the key to a full recovery.
Folk remedies
- Strengthening tea
Mix St. John's wort, peppermint and lemon balm in proportions 3:2:1. Pour 50 g of the mixture into 200 g of boiling water. Leave for half an hour. Drink 1 glass twice a day.
- Calming tincture
Cut and blend 10 lemons, including the peel, in a blender. In a mortar, crush the shells of 5 chicken eggs. Combine them and pour in 0.5 liters of vodka. Leave for 2 days. Drink 2 tbsp. l. three times a day.
- Anti-anxiety infusion
Mix thyme, motherwort and oregano in equal quantities. Pour 50 g of the mixture into 0.5 liters of boiling water. Leave for 4 hours. Drink 1 tbsp. l. three times a day.

The use of folk remedies for ANS lability must be agreed upon with the attending physician and the main course of therapy.
What can happen with lability
The patient has confused thinking. The seriousness of the situation lies in the problem that these people periodically do not realize their actions. They do not differentiate between right and wrong actions. If a sick person conceives something, he brings it to life, even when the act is illegal. Lability of consciousness is caused by depressive psychosis.
Typical in this situation:
- incomprehensible laughter that appears suddenly,
- strange humor,
- excessive gesticulation
- words that are not related to the essence of the conversation,
- confused speech
- lack of focus on certain things.
Since the disease relates to the psychological sphere, doctors in the relevant field say that vegetative lability can be a consequence of some pathology, when the patient feels severe weakness and helplessness and is unable to “fight” the problems surrounding him. In addition, lability
sometimes due to an incorrect upbringing process.
Signs
They are easy to identify when communicating with a person. When he does not admit the obvious and refuses proper therapy, you should try to convince him of the need to turn to specialists.
- Groundless change of mood. In a normal situation, a person may begin to cry, become angry, or laugh.
- Uncertainty, inability to assess your condition. The patient talks about himself either pretentiously or vice versa. When you look at it from the side, you immediately notice deviations in behavior.
- Complete confusion, in a state of instability. A person does not control himself: restless, fussy, overly sensitive.