Entire site Library Scientific articles Consilium Medicum
V.E.Medvedev, F.Yu.Kopylov, E.A.Makukh
Depressive conditions are the most common form of mental pathology in patients of general medical (and especially cardiological) institutions, both outpatient and hospital. The incidence of depression in these patients ranges from 20 to 45% [1-5].
The spectrum of affective disorders in cardiac patients is very diverse: along with nosogenic depression and psychogenic states not associated with the stressogenic effects of somatic illness, hypothymic states are identified due to various biological factors (the reproductive cycle of women, the dynamics of somatic pathology), as well as phases of seasonal affective disorder with the dominance of somatovegetative symptoms , autochthonously occurring endogenous depressions [1, 2, 6-8].
It has been established that the drugs of choice for the treatment of affective disorders in cardiac patients are antidepressants from the group of selective serotonin reuptake inhibitors (SSRIs), comparable to tricyclic antidepressants (TCAs) in effectiveness, but practically free of their negative side effects [9–16]. Accordingly, the development and introduction of a large number of SSRI antidepressants and their generic modifications expand the possibility of selecting a drug that is most appropriate not only for the psychopathological features of depression, but also for concomitant somatic pathology. At the same time, such characteristics of the thymoanaleptic as tolerability and safety come to the fore.
In most psychopharmacological studies, the assessment of these parameters is based on a synthesis of data on the side effects of antidepressants obtained during the study of drugs in somatically well patients. The accumulation of data on the use of generic thymoanaleptics in patients with somatic diseases is aimed at the study program of such psychotropic drugs, carried out by employees of the department for the study of borderline mental pathology (head - academician of the Russian Academy of Medical Sciences A.B. Smulevich) of the National Center for Mental Health of the Russian Academy of Medical Sciences (director - academician RAMS A.S. Tiganov) and the Cardiology Clinic (headed by Prof. A.L. Syrkin) MMA named after. I.M. Sechenova (rector - academician of the RAS and RAMS M.A. Paltsev). During the implementation of this program, a study was conducted on the tolerability, safety and effectiveness of Plisil (paroxetine), one of the SSRIs with somatotropic effects. Thus, according to a number of studies, paroxetine helps reduce platelet aggregation, which prevents thrombus formation and has a protective effect on the vascular endothelium [2, 10, 12], in addition, unlike antidepressants that inhibit the uptake of norepinephrine, paroxetine suppresses antihypertension much weaker - positive effects of guanethidine and helps improve the regulation of the cardiovascular system [12].
Paroxetine is well absorbed and metabolized after the first passage through the liver. The main metabolites of paroxetine are polar and conjugated oxidation and methylation products that are quickly eliminated from the body, have weak pharmacological activity and do not affect its therapeutic effect. When paroxetine is metabolized, the selective uptake of serotonin by neurons due to its action is not impaired.
Equilibrium concentration is achieved by 7-14 days after the start of treatment. Urinary excretion of unchanged paroxetine is usually less than 2% of the dose, with metabolites accounting for about 64%; the intestines excrete about 36% of the dose. The half-life varies, but is usually around 16-21 hours.
Data regarding the use of generic paroxetine in cardiac patients are scarce [17-19] and do not include information on the effect of the drug on basic hemodynamic parameters, but it can be assumed that Plisil will be an effective treatment for depression in patients with cardiovascular pathology, including particularly with arterial hypertension (AH).
Study design
The prospective study included men and women aged 18 to 60 years who were undergoing inpatient or outpatient treatment at the Cardiology Clinic of the MMA named after. I.M. Sechenov with documented hypertension of 1-11 degrees as part of hypertension. All patients met the following criteria: presence of depression meeting the ICD-10 diagnostic criteria for affective disorders (P3.0-B3.9); the need for thymoanaleptic therapy; informed consent to participate in the study. The sample included patients with stable somatic indicators and selected doses of somatotropic therapy [diuretics (hypothiazide, 21 observations), ACE inhibitors (enalapril, 11 observations), calcium antagonists (amlodipine, 8 observations), β-blockers (metoprolol, 6 observations), acetylsalicylic acid (12 observations), prolonged nitrates (isosorbide dinitrate, 3 observations)], established at least 2 weeks before the patient was included in the study.
Patients with manifest schizophrenia and chronic delusional disorders were excluded; patients with signs of dependence on psychoactive substances; organic lesions of the central nervous system; a tendency to allergic reactions (including a history of verified signs of hypersensitivity to paroxetine); history of seizures; pregnant and lactating women, as well as patients who took part in any studies during the 8 weeks preceding this study. Patients with signs of a severe or unstable somatic condition (hepatic and/or renal, heart failure, diseases of the cardiovascular system with a tendency to hypotension and/or orthostatic symptoms, acute coronary syndrome, angina pectoris of III-IV functional class - FC) were also excluded. secondary forms of hypertension, valvular heart defects, cardiac rhythm and conduction disorders, malignant neoplasms).
Plizil was prescribed for 4 weeks 1–3 times a day before meals. The daily dose during the first 5 days of therapy was: 10 mg (days 1-2), 20 mg (days 3-5). Starting on the 6th day of therapy, the dose was titrated individually to an effective dose, ranging from 20 to 60 mg/day, with an average dose of 40 mg/day.
The dynamics of the patients' condition were recorded during 4 weekly visits. Methods for assessing the status of patients were standard rating scales (Hamilton Depression Rating Scale - HDRS and Clinical Global Impression - CGI). Efficacy criteria included a 50% or more reduction from baseline in mean HDRS score, CGI-I scores of “significant improvement” or “major improvement,” and CGI-S scores <2 (“no symptoms” or “borderline”). disorder").
Before the prescription of an antidepressant and after the end of therapy, 24-hour blood pressure (BP) monitoring was performed, as well as 24-hour ECG monitoring according to Holter. The safety of Plisil in relation to the cardiovascular system was assessed both by registered side effects and by the dynamics of average blood pressure values during the day and night, and the indicators of daily ECG monitoring during the first and repeated monitoring, respectively. The UKU Side Effects Scale was used to verify side effects.
To assess the risk of drug interactions between Plizil and somatotropic drugs, cases of increased/manifestation of undesirable effects of Plizil and cardiotropic drugs, potentially associated with changes in the metabolism of one drug under the influence of another, prescribed as part of combination pharmacotherapy, were recorded.
The study excluded the use of other psychotropic medications. In case of severe insomnia, the administration of short-acting hypnotics (zolpi-dem, zopiclone) was additionally allowed. Statistica software (StatSoft, USA) was used for statistical data processing. The significance of differences was assessed using the Kolmogorov-Smirnov test.
Rules for use and contraindications for the drug "Capoten"
Headache (cephalalgia) is a typical symptom of high blood pressure. Tablets for headaches with high blood pressure act both directly on pain sensitivity and on the causes that caused it. This may include increased blood pressure, constriction of blood vessels, tension in the muscles of the face and head, neuralgia, and inflammation of the sinuses. For hypertensive patients, pain in the head is a signal of an attack of hypertension.
Headache with high blood pressure has many mechanisms of development. The increase in pressure is caused by hypertonicity of the sympatho-adrenal system, which produces several pathogenetic effects:
- Increased heart rate and increased stroke volume, as a result of which the vessels of the periphery (including the head) experience increased stress.
- The sympatho-adrenal system works in parallel with the renin-angiotensin-aldosterone system, which increases the hydrophilicity of tissues, including the brain. This leads to local fluid retention in the brain tissue and plasmatic impregnation and hyalinosis of the walls of brain vessels. There is a danger of interstitial cerebral edema.
- The sympathetic nervous system and adrenaline increase blood clotting, which leads to adhesion of formed elements and thrombosis, disruption of the trophism of neurons and glial tissue (intercellular substance in the brain), and irritation of pain receptors.
Relief from pain syndrome is ensured by symptomatic treatment - taking painkillers (Analgin, Nimesil, Baralgin). For headaches caused by high blood pressure, medications that normalize blood pressure are indicated simultaneously with painkillers.
Painkillers belong to the class of non-steroidal anti-inflammatory drugs and analgesics.
Analgesics and NSAIDs block the formation of pain mediators - prostaglandins. Non-steroidal anti-inflammatory tablets, in addition to the analgesic effect, reduce the risk of blood clots, which leads to improved blood circulation. However, for moderate and severe hypertension, it is dangerous to use such drugs, especially for older people, due to loss of vascular elasticity and the risk of hemorrhagic stroke.
In hypertension or symptomatic hypertension, headache is caused by increased hemodynamic pressure on the blood vessels. Reducing blood (and intracranial) pressure will help relieve discomfort.
Sample characteristics
30 patients (11 men, 19 women, mean age 49.4±1.7 years) received Plysil. The average duration of hypertension at the time of examination was 6.2±2.4 years.
Analysis of the sociodemographic characteristics of the patients made it possible to establish that the majority of them (25 observations) retained full ability to work (worked or studied); 23 had a stable marital status. 5 patients did not work (of which 1 was due to a disability associated with a somatic disease, 4 due to age). The absence of significant changes in social status indirectly indicated a favorable course of somatic disease, which was confirmed by physical examination data.
Psychopathological disorders were represented by nosogenic depression (hypotymic reactions to a set of psychotraumatic factors associated with a somatic illness) - 19 observations, dysthymic disorder - 6 observations, endogenous depression - 5 observations.
Regardless of the diagnostic classification of depression, the phenomena of negative affectivity—apathy, anhedonia—predominated in the patients studied. Patients noted lethargy, depression with chest tightness, unusual for their everyday state, and a feeling of internal discomfort. Only 5 observations revealed the circadian rhythm characteristic of most vital depressions (feeling most painful in the morning hours). The content complex of depression was expressed by hypochondriacal ideas (thoughts about the futility of treatment, the unfavorable outcome of cardiovascular pathology, its irreparable social consequences). A significant place in the structure of the affective syndrome was occupied by somatovegetative manifestations, which were realized, as a rule, in the form of homonomic (reminiscent of symptoms of cardiovascular pathology) somatization and conversion symptoms.
Premorbid characteristics of patients with hypertension and depressive disorders were represented by anomalies of hysterical (12 observations), obsessive-compulsive (10 observations, including anxiety - 7 and anancastic -3), affective (hyperthymic -3 observations), borderline (BPD) and paranoid (2 observations each), dependent (1 observation) circle.
Somatic pathology in the studied sample was represented by hypertension stages I and II (VNOK Recommendations, 2004) - 17 and 13 observations, respectively. The maximum rise in blood pressure was 170.4±12.3 mm Hg. Art. for systolic and 112.1±1b.7 mmHg. Art. for diastolic at a relatively low “working” blood pressure (131.4 and 72.1 mm Hg, respectively). In 28 observations, no complications of hypertension were noted. The moderate nature of the course of somatic pathology was also evidenced by the data of an echocardiographic study. In 16 observations, no signs of left ventricular (LV) myocardial hypertrophy or disturbances in its local and/or general contractility were identified. Angina pectoris FC 1-11 was verified in 11 cases; it was characterized by typical attacks under moderate stress.
ANTIDEPRESSANTS FOR HYPERTENSION
— individual and group psychotherapy for personal growth —
training for anxiety management and successful communication.
I recommend – Rehabilitation Medicine Clinic
May God grant you never have any reason to see a doctor!
And if you have to, don’t delay it.
Hypertension is a psychosomatic disease. This means that its onset and exacerbations can be associated with emotional experiences, irritability, anger, and resentment. So the help of a psychotherapist, but not a neurologist, will help stabilize your condition.
Antidepressants are used not only for depression, but also for other mental and psychosomatic disorders.
- If you have questions for the consultant, ask him via a personal message or use the “Ask a Question” form on the pages of our website.
results
Efficacy of therapy
Of the 30 patients included in the study, 29 completed the study. The number of responders (according to the criteria adopted in the study) was 18 out of 30. According to the SON scale, 10 patients had “marked improvement” in 8 patients. Another 4 patients showed “moderate improvement” in CO1-1.
Similar results were obtained when analyzing the dynamics of the severity of psychopathological disorders on the CO1^ scale. At the time of final assessment, the initial mean SOC score (3.9) had decreased to 1.9 or lower in 19 cases (Fig. 1).
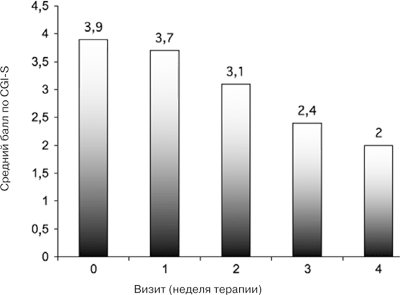
Rice. 1. Dynamics of average CGI-S scores during 4 weeks of Plizil therapy in the studied sample (n=30).
A clear reduction in psychopathological symptoms was recorded mainly in patients with nosogenic depression (15 observations). The decrease in the severity of symptoms of endogenous depression and dysthymia was moderate (2 and 1 observation, respectively).
The pronounced clinical effect of Plizil, established by the effectiveness criterion (SON and SOK scales), was confirmed by a significant reduction in the initial depression scores on the NBCE scale (Fig. 2). The reverse development of depressive symptoms begins in the 2nd week of treatment and becomes more pronounced with further therapy, with continuous improvement in indicators until the last (4th) week of therapy (p<0.005). Clinically, this is manifested by a decrease in the severity of hypothymia and a reduction in the depressive content complex. Patients note an improvement in mood with a simultaneous decrease in lethargy, depression, and emotional tension. Hypochondriacal ideas were de-actualized. Noting the restoration of their previous mental balance, patients state that until recently they assessed the situation too pessimistically and “unconsciously” exaggerated the danger of the disease.
Rice. 2. Dynamics of the average total anxiety scores on the HDRS scale during 4 weeks of Plizil therapy in the studied sample (n=30).
During a somatic examination during the study, it was found that during treatment with Plizil in combination with antihypertensive therapy, the average systolic blood pressure during the daytime (from 8 to 23 hours) significantly decreased from 144±3.2 to 133±1.9 mmHg . Art. (p<0.05), and at night (from 11 p.m. to 8 a.m.) - from 126±1.2 to 120±1.1 mm Hg. Art. (p<0.05) respectively. Similar results were obtained for diastolic blood pressure: its level decreased during the daytime from 79±2.5 to 73±2.1 mm Hg. Art. (p<0.05), and at night - from 76±1.3 to 71±2.1 mm Hg. Art. (p<0.05).
Regarding the results of Holter monitoring, it can be noted that there are no significant differences in the indicators of supraventricular and ventricular ectopic activity, as well as the dynamics of the ST segment. You should also pay attention to the lack of dynamics of the QT and QTc intervals while taking the drug, which is important due to the undesirable property of a number of antidepressants, in particular TCAs, - the ability to prolong the QT interval and cause life-threatening ventricular tachycardias such as torsades de pointes.
Tolerability of therapy
The fact that 29 patients completed the full course of treatment confirms the literature data on the safety of the drug. One patient stopped taking Plisil in the 1st week of treatment due to severe nausea and daytime sleepiness. In another 9 patients, these side effects were moderate and did not require discontinuation of the drug. The results obtained are fully consistent with the data that among the side effects of paroxetine, nausea and moderate sedation are most often mentioned [11-15].
Other adverse events during Plizil therapy were recorded in 6 patients: 2 observations each - early insomnia in the 1st-2nd week, decreased appetite during the first 2 weeks of taking the drug and a change in taste in the 2nd week of treatment. Side effects manifested mainly during the first 2 weeks of therapy and usually stopped as depressive symptoms reversed or the drug dose was adjusted. A cardiologically favorable safety profile of the drug has been established. None of the observations recorded clinically significant interactions between the studied antidepressant and drugs aimed at correcting cardiovascular pathology. At the end of therapy, no life-threatening arrhythmias and/or intracardiac blockades were recorded in the patients of the studied sample. The study did not detect any effect of Plizil on blood counts.
Features of treatment of depression in hypertensive patients
The most important thing is to seek professional help from a doctor.
Treatment of a depressive state against the background of high blood pressure requires complex therapy, which is aimed at simultaneous normalization of mental and physiological health. Both pathologies have an unstable course, so exacerbations can occur in the shortest possible time. It is very important not to self-medicate, which can lead to disastrous consequences.
- sedatives;
- antidepressants;
- tranquilizers;
- drugs to normalize blood pressure;
- vitamin complexes.
In advanced stages, it is difficult to do without consulting a psychotherapist. Without normalization of the psycho-emotional state, treatment of hypertension will not be effective. Additional methods include yoga, meditation, physical therapy, and breathing exercises. Much attention should be paid to sleep and rest. It is important that during the therapy the patient is in a positive atmosphere; he needs care and comfort.
Mechanism of action
For patients suffering from depression, antidepressants help them return to life. Their appetite and mood improve, melancholy and despondency disappear, and insomnia disappears.
It should be noted that these medications only affect the patient suffering from depression.
Healthy people will not feel any changes in their well-being unless they are experiencing side effects from antidepressants.