Research
Some of the advanced strategies include: introduction of the dystrophin gene;
changing the way cells interpret dystrophin gene instructions; correction of the gene itself; management of other body proteins to compensate for the absence/lack of dystrophin; improvement of steroid drugs, and the use of stem cells to restore damaged muscles1. Other studies are focusing on treating heart failure associated with dystrophin deficiency.
Damage to the dystrophin gene leads to Duchenne muscular dystrophy (DMD), in the same way as the less severe form, Becker muscular dystrophy (BMD). Many treatment strategies tried in DMD are applicable to Becker muscular dystrophy.
To learn more about research on BMD, check out these videos: Clinical Studies of Muscular Dystrophy in Animal Models and BMD: From Targets to Clinical Trials.
Cardiac support
Researchers are pursuing several strategies to support and improve cardiac function in BMD and DMD. They mainly test existing drugs for possible benefit to the heart affected by DMD and BMD and conduct research to understand and find new approaches to treating the heart in these diseases.
In 2009, researchers found that mutations in the dystrophin gene that cause cardiomyopathy in BMD may not affect regions of the protein responsible for skeletal muscle loss. Research may allow better prediction of the onset of cardiomyopathy in BMD and the use of cardioprotective therapy at earlier stages. They also give researchers insight into which parts of the protein need to be preserved when considering truncated dystrophin molecules as therapeutic strategies.
The drug sildenafil (Viagra) has been found to have a cardioprotective effect in mice with both early and late stage DMD-like disease. Sildenafil, used to treat erectile dysfunction, belongs to the phosphodiesterase-5 (PDE5) inhibitor class. It relaxes the smooth muscle lining blood vessels, increasing blood flow to the muscles and heart. The cardiac effects of sildenafil in adolescents and men with DMD are being studied.
Laboratory studies have shown that an experimental compound designed to seal cell membranes, p 188, improves heart function in dogs with dystrophin deficiency.
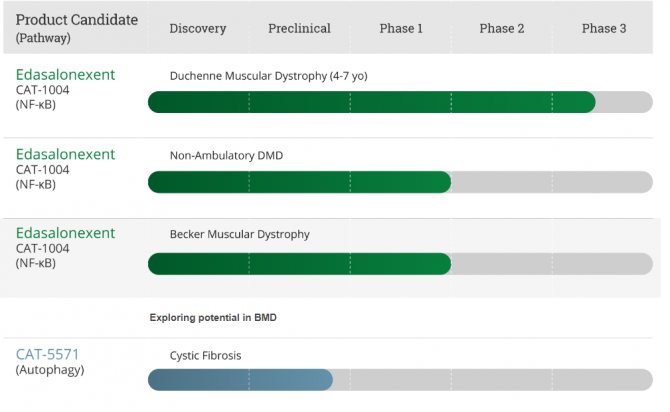
In 2011, MDA-supported researchers found that inhibiting the action of the NF-kappa B protein improved cardiac function in mice with severe DMD-like disease. The pharmaceutical company Catabasis provides infographic material on its official website about the drug Edasalonexent (CAT-1004), an inhibitor of the NF-kappa B protein.
Catabasis research schedule
According to the information presented in this graphic, the potential of Edasalonexent (CAT-1004) in the treatment of BMD2 is currently being studied.
Treatment of progressive Becker muscular dystrophy
- Symptomatic therapy.
- Dosed exercise therapy.
- Glucocorticosteroids.
- Surgical treatment of contractures.
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist.
Essential drugs
There are contraindications. Specialist consultation is required.
- Prednisolone (systemic glucocorticosteroid). Dosage regimen: orally, at a dose of 20-80 mg/day. for 3-4 doses. Maintenance dose 5-10 mg/day.
- Methylandrostenediol (anabolic steroid). Dosage regimen: sublingually, adults at a dose of 0.025–0.050 g/day, children at a dose of 1.0–1.5 mg/kg/day. for 3-4 doses.
- ATP (a drug that improves muscle trophism). Dosage regimen: intramuscularly, in a dose of 1 ml of 1% solution 1–2 times a day. For a course of treatment - 30–40 injections. Repeated course - after 1–2 months.
Gene editing - CRISPR/Cas9
The CRISPR/Cas9 method is based on the natural defense system of bacteria against viral infection (analogous to the immune system). When a bacterium detects the presence of foreign (in this case, viral) DNA, the CRISPR protein grabs part of the viral DNA and inserts this fragment into the bacterium's own genome. The bacteria then use the “immunizing” piece of viral DNA to produce “antibodies” that recognize and protect against future viral attacks3.
Bacterial “antibodies” include two types of short RNAs that form a complex with the Cas9 protein. Cas9 is a nuclease (a type of enzyme that can cut DNA). When the virus's matching nucleotide sequence (guide RNA) detects a target in the virus's genome, Cas9 cuts the viral DNA, sequestering the virus and preventing it from replicating.
How could CRISPR/Cas9 be used to treat muscular dystrophy?
The CRISPR/Cas9 system can be used to change or correct mutations in patient cells. Researchers are working to find the best way to treat different types of muscular dystrophy (and other genetic diseases) using this method.
The first human clinical trials of CRISPR/Cas9 to treat diseases such as cancer or cystic fibrosis are in development. In these trials, a patient's cells are isolated, treated to correct the genetic mutation, and then injected back into the patient to fight the disease.
For muscular dystrophy, a viral delivery system could provide patient cells with instructions to synthesize the Cas9 protein, as well as guide RNAs that target specific regions of DNA.
Let's look at the example of mice with DMD. The disease is caused by mutations in the gene that contains instructions for producing dystrophin. After treatment with the CRISPR/Cas9 system, it was possible to restore the function of dystrophin in muscle cells of mice.
Similar preclinical studies are being conducted to evaluate the potential of the CRISPR/Cas9 system to treat other types of muscular dystrophy.
For detailed information, more than 200 articles on CRISPR/cas-9 are available for review on the Biomolecule journal website https://biomolecula.ru/search/crispr
Gene therapy
Gene therapy, or gene transfer, refers to the delivery of genes as therapeutic agents. Since the genes contain instructions for protein synthesis, this would directly or indirectly be considered a therapy for neuromuscular diseases. Because the transferred genes can potentially continue to produce protein for some time, gene therapy may offer a more reliable solution than other treatments. However, gene therapy faces many technical challenges, as well as special controls imposed by regulatory agencies such as the US Food and Drug Administration (FDA), that prevent gene therapy from being a clinically applicable method at present.
Key challenges are delivering genes to the target tissue while avoiding unwanted tissues and unwanted immune responses to proteins derived from new genes or to delivery vehicles for new genes.
Scientists with MDA support created a reduced working dystrophin gene, which was tested in boys with DMD. Although the treatment seemed safe, some of the boys experienced an unwanted immune response to the dystrophin protein, which limited the efficiency of the gene transfer. This immune response is being further studied.
Causes of Duchenne dystrophy
The cause of the disease is a congenital defect of the sex X chromosome. The gene that is responsible for the production of muscle protein in the body, dystrophin, is affected. It is the basis of all muscle fibers at the cellular level. The substance is necessary for the correct development of the skeleton, the ability of muscles to contract and relax many times in a row.
In Duchenne disease, the protein is completely absent or defective, that is, it does not perform its function. It is replaced by fatty or connective tissue, making movement impossible.
The disease has a recessive type of inheritance, linked to the X chromosome, and occurs due to mutations in both paired carriers. The pathology mainly affects boys, since they have one X chromosome in their genetic makeup. If it is defective, then the disease occurs.
Myostatin inhibition
Blocking the myostatin protein using the follistatin protein is a strategy that has potential for the treatment of DMD and likely many other neuromuscular diseases. Mice with a DMD-like disease given follistatin protein genes showed an overall increase in body weight and individual muscle weight. The monkeys that received the follistatin gene transfer had stronger and larger muscles.
A strategy that has received significant support from MDA is to inhibit the action of the naturally occurring muscle growth-limiting protein myostatin. Researchers hope that blocking myostatin may allow muscles to grow bigger and stronger.
Myostatin inhibitors have received much attention in the neuromuscular disease research community since it was discovered several years ago that humans and animals with genetic myostatin deficiency have large muscles and good strength without apparent side effects. A 2010 study found that mice lacking dystrophin and having a disease similar to DMD benefited from treatment with a “bait” that lured myostatin out of their muscles.
The biotech company Acceleron Pharma then developed a drug based on this bait and began testing it with MDA support in boys with DMD. Unfortunately, unexpected safety issues arose during this trial, causing Acceleron to discontinue it in 2011.
The company hopes to resolve these safety issues and resume testing of ACE-031 or a modified version of ACE-031.
The results of the ACE-031 study for patients with DMD4 can be found on Clinicaltrials.gov.
Other strategies for myostatin inhibition, such as gene injection for the myostatin-blocking follistatin, are also under consideration.
Stem cells
Stem cells are cells in the earliest stages of development. They can develop into a special type of cell (such as muscle or nerve cells), or retain pluripotency—the ability to develop into any of a number of different cell types.
Stem cell transplantation is proposed as a treatment for diseases such as muscular dystrophy. Cell-based therapies have attempted to stimulate muscle regeneration with the hope that stem cells will restore muscle function and correct pathology by re-synthesizing muscle. Stem cells are considered as a suitable option for therapeutic applications due to their self-renewal ability and differentiation potential.
In 2006, researchers supported by the Muscular Dystrophy Association (MDA) restored mobility in two dogs and stabilized function in a third using stem cells taken from muscle blood vessels.
In a study published in 2007, a European research team successfully used a combination of genetic editing and stem cells to treat mice with DMD. Researchers in this study extracted muscle-generating stem cells from muscle tissue and blood from people with DMD, corrected a genetic error in the cells' dystrophin genes, and then injected the cells into dystrophin-deficient mice. Muscle-derived cells induced better muscle regeneration than blood-derived cells.
In 2010, French scientists, supported by the MDA, reported that they had identified a previously unknown type of muscle stem cells located in the spaces between muscle fibers in mice. Although this is still in the early stages of research, there is hope that the new cells, called PICs, may play an important role in muscle regeneration and repair.
That same year, researchers claimed that the formation of new muscle tissue first required a controlled type of DNA damage. The new discovery has expanded scientists' understanding of how immature muscle cells become muscle and helped them manipulate the process to treat several forms of muscular dystrophy.
Stem cells continue to be a major area of research for specialists and researchers in the field of neuromuscular diseases. Some continue to study muscle satellite cells, a type of stem cell found in muscle tissue. Others are studying different types of cells that can survive transplantation into muscle and produce the desired proteins. In addition, similarities and differences in the development of skeletal muscle and adipose tissue are studied.
In recent years (from 2013 to 2020), encouraging results have been obtained in human treatment using mature stem cells. So prof. Sharma, with the participation of co-authors., in 2013, studied the effect of intramuscular autotransplantation of bone marrow mesenchymal stem cells in 150 patients with muscular dystrophy (meaning stem cells. After 12 months of follow-up, patients showed an increase in muscle strength and improvement in gait. Symptomatic and functional improvements were also observed in 86.67% of cases: in six patients the level of fatty infiltration was reduced and muscle regeneration was detected on MRI images, and in nine patients positive changes in the electrical activity of muscles were detected on electroneuromyography (ENMG).
Mesanchymal stem cells are composed of a variety of cells, such as hematopoietic stem cells, tissue-specific progenitor cells, stromal cells and specialized blood cells at different stages of development5. These cells have the ability to mobilize and exert their reparative effects at the site of injury. They promote neovascularization and enhance angiogenesis (vascular formation) by producing signaling molecules such as vascular endothelial growth factors and fibroblast growth factors (FGF2). They also promote tissue remodeling, prevent apoptosis (cell death), reduce inflammation, release growth factors, and activate satellite cells. These are paracrine effects that can help achieve the desired outcome of cell therapy6,7. Autologous bone marrow mesenchymal stem cells were used in this case because they have no ethical issues and their safety has been established (no donor required, these are the patient's own cells).
Transplanting stem cells into the desired location in the muscle body is usually a major practical difficulty. Intravenous administration of bone marrow-derived stem cells has shown successful re-entry of stem cells into damaged muscle tissue in animal models; however, this also risks diluting the cell concentration. Muscular dystrophy is primarily perceived as a muscle disorder, with little evidence of neuromuscular involvement. Dystrophin is part of a structural protein found in myelin that forms Schwann cells and nerves. Demyelination and degeneration as changes in nerves can occur with such disturbances in cells. Therefore, two different methods of cell transplantation were chosen: intramuscular and intrathecal. Bone marrow mesenchymal cells were injected into the motor points of targeted weak muscles to restore the innervating nerve as well as the muscles. Cerebrospinal fluid is known to contain growth factors that help the growth of cortical epithelium and stimulate vascularization in the nervous system, so it has been used as a dilution medium.
Of particular interest is the clinical case of a patient with Becker muscular dystrophy, who was treated with bone marrow mesanchymal cells.
The results were encouraging. After cell therapy, the patient was observed twice in the hospital at 3 and 9 months. After 3 months, improvement in motor function of the upper extremities was noted. Performing overhead movements required comparatively less effort. Bilateral reduction in gastrocnemius muscle stiffness and pseudohypertrophy was observed. There were significant improvements in standing and sitting position, and in the ability to maintain balance. Balance while standing and walking has improved. The frequency of falls while walking decreased markedly from 4-5 falls per month to 1 fall per 3 months. Characteristics of respiratory function also improved: vital capacity (VC) (from 1250 ml to 1750 ml) and peak expiratory flow (PEF) (from 290 ml to 360 ml).
For more details, read the entry “Efficacy of cell therapy in progressive Becker muscular dystrophy”8.
Symptoms
The onset of the disease occurs between the ages of 5 and 15 years, but can be much later, after 40 years. The first signs are increased fatigue and muscle weakness in the pelvis and lower extremities. Some patients experience periodic and spontaneous cramps of the calf muscles. It is difficult to climb stairs, stand up and sit down, and when trying to get up from a chair you have to look for a support point. The so-called Govers symptom may occur, when a person seems to step his hands along the surface of his legs, thus helping the body straighten.
Pain and cramps in the leg muscles are a characteristic sign of myopathy
All hereditary myopathies are characterized by a symmetrical development of muscle atrophy. First, the thigh muscles and pelvic area are affected, later the process moves to the muscles of the shoulders and upper arms. At the initial stages, pseudohypertrophy is formed in the calf muscles, later they are joined by the deltoid, triceps and quadriceps muscles (quadriceps femoris). Subsequently, pseudohypertrophy is transformed into muscle wasting.
Symptoms of Becker myopathy are expressed:
- heart rhythm disturbances - arrhythmia;
- pain in the muscles of the arms and legs, as well as other parts of the body;
- pain in the legs increases when walking;
- the gait acquires new features and becomes like a duck’s;
- constant twitching is felt in the leg muscles;
- it becomes increasingly difficult to move normally and avoid obstacles;
- even minor physical activity is accompanied by shortness of breath and fatigue, as well as swelling of the legs.
The full range of symptoms is rarely present in one patient, but fatigue and weakness in the legs are felt by absolutely all patients.
The peculiarity of Becker's myopathy is that it progresses quite slowly, but in any case leads to immobility and stiffness of the joints. The process continues until about 40 years of age; upon reaching this age, physical activity usually stops. It should be noted that skeletal deformities, such as spinal curvature, do not occur. Brain activity remains normal, the heart and blood vessels are mildly affected. In some cases, impotence and decreased sexual desire are possible, and sometimes gynecomastia and testicular atrophy are observed.
utrophin enhancement
Laboratory data indicate that increasing levels of the muscle protein utrophin may, to some extent, compensate for dystrophin deficiency.
Utrophin is very similar to dystrophin, but unlike dystrophin, it is normally produced and fully functional in BMD. Therefore, increasing utrophin levels is unlikely to cause an unwanted immune response, whereas increasing dystrophin levels may. Increasing utrophin production may help compensate for dystrophin deficiency regardless of the specific dystrophin gene mutation.
Although utrophin is similar in structure and function to dystrophin, there is at least one key difference between the two proteins. During fetal development and perhaps a little later, utrophin is present throughout the muscle fiber, interacting with clusters of proteins trapped in the surrounding membrane. As an animal or person ages, utrophin is almost completely replaced by dystrophin, with one exception. Utrophine remains at the neuromuscular junction throughout life.
Several strategies are currently attempting to increase utrophin. One of them is to identify and suppress everything that interferes with the production of utrophin - find the brake and, so to speak, release it.
Another strategy is to introduce a modified version of the utrophin protein itself into the body. A 2009 study found that a modified utrophin protein provided significant benefits when administered to mice that lack the dystrophin protein and have a disease resembling DMD.
In 2011, scientists reported that systemically administering a human form of a protein called biglycan to mice with a disease like DMD increased muscle resistance to damage associated with muscle contraction.
Biography
In 1894 he entered the School of Military Medical Service in Lyon. In 1897, he submitted a dissertation for his doctorate on the “antagonism between mold and microbes.”
Duchesne sent his thesis to the Pasteur Institute, but received no response. He considered it necessary to continue research, but further military service prevented this.
He spent one year in internship in Val-de-Grâce, then was appointed major of medicine 2nd class in the 2nd Hussars in Senlis.
In 1901 he got married. Two years later, the wife died of tuberculosis.
In 1904 he fell ill with a severe chest illness (presumably tuberculosis). Three years later he was dismissed from military service and sent to a sanatorium in Amelie-les-Bains.
Died April 12, 1912, aged 37. He was buried next to his wife in the Grand Jas cemetery in Cannes.