Schizencephaly is a rare congenital brain disorder in which abnormal fissures or clefts form in the hemispheres of the brain.
Signs and symptoms of this disease may include developmental delays, seizures, and problems with the blood supply to the spinal cord. People suffering from this pathology may also have an abnormally small head (microcephaly); hydrocephalus; intellectual underdevelopment; partial or complete paralysis; and/or poor muscle tone (hypotonia).
The severity of symptoms depends on many factors, including the extent of the splitting and the presence or absence of other brain abnormalities. Although the exact cause of schizencephaly is unknown, it is associated with various genetic and non-genetic factors. Treatment usually consists of physical therapy and medications to prevent seizures. In cases complicated by hydrocephalus, a surgically implanted tube called a shunt is often used to divert fluid to another area of the body where it can be absorbed.
Signs and symptoms of schizencephaly
These signs of anomaly include:
- Developmental delay;
- Seizures;
- Abnormally small head (microcephaly);
- Intellectual underdevelopment;
- Partial or complete paralysis;
- Weak muscle tone (hypotonia);
- Hydrocephalus
The severity of the disease's symptoms depends on many factors, including the degree of splitting and the presence of other brain abnormalities. For example, small clefts in one hemisphere of the brain can lead to paralysis on one side of the body, but people can be almost fully mentally developed, while clefts in both hemispheres of the brain can lead to quadriplegia (paralysis of both arms and legs) and severe intellectual disability .
Therapy methods
Treatment of cerebral schizencephaly can only be symptomatic. This defect cannot be corrected surgically.
For epileptic seizures, anticonvulsant medications are prescribed:
- "Finlepsin".
- "Depakine."
- "Convulex".
In mild cases, taking antiepileptic drugs leads to complete disappearance of seizures.
In more severe forms of the pathology, the administration of drugs based on botulinum toxin helps stop seizures. They slow down the transmission of signals from nerves to muscles and reduce the frequency of attacks.
If the patient has cognitive impairment, then sessions of electrical stimulation of the brain are prescribed. The procedures help increase the activity of the cerebral cortex.
For hydrocephalus, diuretics are indicated:
- "Veroshpirona".
- "Diakarba".
- "Furosemide".
However, diuretics help only temporarily reduce cerebral pressure and alleviate the patient’s condition. A more radical and effective treatment method is bypass surgery. A special tube is inserted into the brain. Through it, the cerebrospinal fluid flows to another part of the body, where it is absorbed.
Be sure to prescribe therapeutic exercises to improve coordination and increase muscle tone. Exercises also help restore movement in case of paralysis and paresis. Sick children need developmental classes with a speech therapist. An occupational therapist may need to help teach the child self-care skills.
Causes
The exact cause of schizencephaly is unknown. A small number of people with schizencephaly have been found to have changes (mutations) in one of four genes: EMX2, SIX3, SHH and COL4A1. Rarely, schizencephaly may affect more than one family member. In some cases, this has genetic reasons.
Schizencephaly has also been associated with various nongenetic factors, including young maternal age and exposure to certain medications, as well as infections, which can cause vascular problems (impaired circulation or blood supply) in the developing child.
Schizencephaly is not considered to be hereditary in most cases and rarely affects more than one person in a family. Several cases of familial schizencephaly have been associated with changes (mutations) in the EMX2 gene.
Diagnostics
In rare cases, people with schizencephaly have changes (mutations) in one of four genes: EMX2, SIX3, SHH and COL4A1.
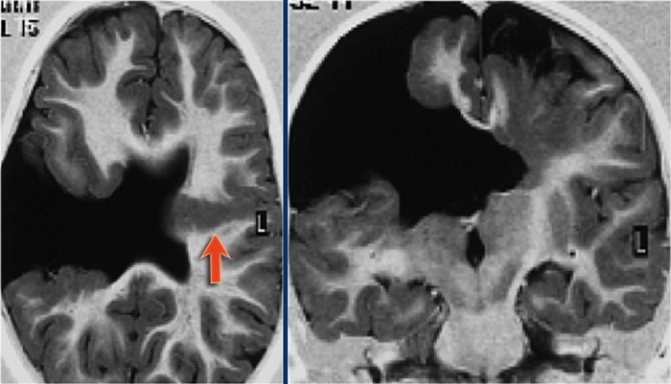
Schizencephaly is usually diagnosed using computed tomography (CT) and/or magnetic resonance imaging (MRI). A CT scan is an imaging technique that uses X-rays to create cross-sectional images of the body, while an MRI scan uses a powerful magnetic field and radio waves to create images of the brain and surrounding nerve tissue. Both of these imaging techniques can be used to identify brain abnormalities, such as fissures or clefts, found in people with schizencephaly.
In some cases, schizencephaly can also be diagnosed prenatally (before birth) by ultrasound after 20 weeks of pregnancy. If a cleft is visible on ultrasound, an MRI scan of the developing child may be recommended to confirm the diagnosis.
Features of schizencephaly, porencephaly, holoprosencephaly
Bilateral cleft of the cerebral hemispheres is formed at the stage of embryogenesis. The morphological structure of the formation can be open or closed.
Unilateral localization of pathology on MRI images may resemble a cyst. Along the cleft there are pathological areas of cerebral parenchyma - microgyria, zones of increased repeated activity, spastic paralysis.
Porencephaly is characterized by the formation of cystic cavities within the cerebral parenchyma. The causes of the pathology are hemorrhage inside the brain, heart attacks, strokes. The typical location of the cyst is the Sylvian fissure.
In rare cases, porencephaly is characterized by the formation of abnormal passages between the cystic cavity and the ventricular spaces. The nosology is often characterized by other stigmas of disembryogenesis:
- Microcephaly;
- Encephalocele;
- Agiriya.
A child with a developmental defect experiences neurological disorders:
- Oligophrenia (mental retardation);
- Epilepsy attacks;
- Atrophic changes in the optic discs;
- Tetraparesis.
Concomitant changes complicate the clinical picture:
- Arterial and venous hemorrhages;
- Intracranial hypertension (in case of impaired circulation of cerebrospinal fluid);
- Cerebral infarctions;
- Hemiparesis;
- Focal epileptic foci.
Pseudoporencephalic cysts often have a unilateral (one-sided) location. They are often combined with defects of the central nervous system and defects in cell migration.
Schizencephaly on MRI
The disease occurs due to the pathological division of the chemical substance prosencephalon.
Classification of nosology by severity:
- Lobarnaya;
- Semi-lobar;
- Alobar.
The heaviest is the last form. With it, a number of congenital anomalies are observed:
- Underdevelopment of the premaxillary bone;
- Sinophthalmos;
- Cebocephaly.
Against the background of multiple anomalies, parts of the face are difficult to distinguish. Associated neuronal migration defects:
- Synostosis (fusion of nerve ganglia);
- Presence of one cerebral ventricle.
The etiological mechanisms of hereditary defects have not been established. Holoprosencephaly is fatal in most cases, but the incomplete form can lead to disability.
Smoothing of the convolutions of the cerebral cortex (agyria) is formed in utero. The pathogenetic mechanism for the development of the nosology is a violation of embryogenesis caused by the pathology of the spread of neuroblasts from the primary neural tube. Smoothing of the surface is accompanied by a decrease in mental and intellectual activity.
Concomitant neurological disorders gradually increase. The disease is fatal in infancy.
The absence of cerebral convolutions excludes the optimal functioning of the second signaling system, which exists only in humans. Folding increases the functional surface of the brain.
Even early detection using MRI cannot save the life of a child with type 1 or type 2 lissencephaly.
During pregnancy, congenital malformations of cerebral structures are determined by ultrasound examination (ultrasound). The reliability of the procedure is 60%, so sometimes congenital malformations of the brain are detected after MRI, although intrauterine monitoring of pathology does not determine pathological conditions.
An example of a magnetic resonance imaging report:
- Bilateral ventriculomegaly;
- Increased liquor spaces;
- Smoothness of the cerebral convolutions;
- Incomplete absence of folds in the parietal and frontotemporal regions;
- Dilatation of the lateral ventricles.
READ MORE: Brain angioma: symptoms and treatment of brain angioma
The nosology is often combined with the stigmas of cerebral dysembryogenesis - macrocephaly, agyria, microcephaly.
Medical sources claim that pathology can be detected by ultrasound after the twenty-sixth week of pregnancy.
MRI: normal and lissencephaly
Lissencephaly type 2 is alternatively called Norman-Roberts syndrome. Canadian scientists who discovered the disease consider the mutation of the “RELN” gene to be the main cause of the disease.
The DNA region responsible for nosology encodes the formation of the “Reelin” protein. The syndrome is characterized by many clinical changes:
- Lymphedema (lymphedema);
- Epileptic seizures;
- Sloping forehead;
- Thickening of the cerebral cortex;
- Agyria (smoothness of the cerebral sulci);
- Macrocephaly;
- Microcephaly.
Perinatal ultrasound detects most cases of the disease.
Treatment
The best treatment options for people with schizencephaly depend on many factors, including the severity of the condition and the signs and symptoms present. For example, people with developmental delay or partial paralysis may receive physical therapy and/or occupational therapy. Medicines are usually prescribed to prevent attacks. In cases complicated by hydrocephalus, a surgically implanted tube called a shunt is often used to divert fluid to another area of the body where it will be absorbed.
Porencephaly
- Definition
- Story
- Morphology
- Differential diagnosis
- Clinical picture
Definition
Porencephalia (porencephalia, Greek: poros - passage, hole, pore + enliephalos - brain) is a pathological cystic expansion of the cerebral ventricle cavity of varying sizes, communicating with the subarachnoid space. In reality, the boundary between porencephaly and schizencephaly is blurred.
Story
The term “porencephaly” was introduced in 1859 by RL Heschl, who described a congenital defect of the cerebral hemispheres, extending from the cerebral cortex to the wall of the lateral ventricle.
In 1969, DD Matson proposed using this term only in relation to cystic cavities of the brain of congenital origin. In neurosurgical practice, this term sometimes refers to an artificially created communication between the subarachnoid space (cavitas subarachnoidalis) and the lateral ventricle of the brain.
Morphology
Porencephaly is a cerebrospinal fluid-containing cavity associated with the subarachnoid space or ventricles of the brain. Porencephaly can be true or false, which are distinguished by the presence or absence of gray matter at the edge of the cleft.
True porencephaly (schizencephaly) is always congenital and involves the existence of clefts in the substance of the brain that connect the ventricle and the subarachnoid space.
Secondary porencephaly is a consequence of trauma, inflammatory processes (meningitis, encephalitis, ventriculitis), cerebrovascular lesions (intracerebral hemorrhage), surgery (including after ventricular puncture, and also occurs due to poor functioning of the shunt).
On CT and MRI images, there is a zone of cerebrospinal fluid density (signal intensity) associated with the ventricle and (or) subarachnoid space. Asymmetrical dilatation of the ventricles with or without displacement beyond the midline, due to the presence of a pressure gradient between the hemispheres. After administration of a contrast agent, there is no increase in signal from the cavity walls. The use of cisternography makes it possible to identify the communication of the cavity with the ventricle or subarachnoid space.
Fig.1
Fig.2
Differential diagnosis
Schizencephaly is usually combined with heterotopia of the gray matter, agenesis of the corpus callosum, etc. The cause is a violation of neural migration and organization of the cortex due to ischemic, toxic lesions of the fetal brain.
MRI makes it quite easy to differentiate between schizencephaly and secondary porennephaly. If in schizencephaly the edges of the cavity are dysplastic, thickened gray matter, then in secondary porencephaly they are white matter. The ability to perform MR cisternography makes MRI the method of choice when examining patients with porencephaly.
A sign that distinguishes porencephaly from abscesses and cystic tumors is the absence of increased signal intensity from the walls of the cavity after intravenous contrast.
Clinical picture
Clinical manifestations depend on the location and size of the brain damage. Children are usually diagnosed with delayed psychomotor development of varying severity, hemiparesis, focal motor seizures, etc. Symptoms are usually unilateral.
Author: radiologist, Ph.D. Vlasov Evgeniy Alexandrovich
Full or partial reprint of this article is permitted by installing an active hyperlink to the source
Similar articles
| Arachnoid cysts An arachnoid cyst is a cerebrospinal fluid cyst, the walls of which are formed by the arachnoid membrane. Arachnoid cysts are located between the surface of the brain and the arachnoid (arachnoid) membrane. |
| Agenesis of the corpus callosum Agenesis of the corpus callosum can be complete or partial. Often accompanied by congenital lipoma and dilatation of the ventricular system. |
| Dandy-Walker Anomaly Dandy-Walker anomaly is complete or partial agenesis of the cerebellar vermis, counterclockwise rotation of the cerebellum with expansion of the fourth ventricle against the background of expansion of the posterior cranial fossa due to upward displacement of the tentorium |
| Heterotopia Heterotopia is a violation of the migration of nerve cells with the formation of pathological zones of gray matter grouping in the white matter |
| Intracranial and spinal lipoma Intracranial lipoma is a benign formation that consists of adipose tissue |
| Pachygyria and lissencephaly Pachygyria is a disorder of the formation of the cerebral cortex with smoothing of the sulci and the appearance of rare massive convolutions |
| Polymicrogyria Polymicrogyria is a congenital anomaly of the development of the cerebral cortex with the formation of multiple small and dense convolutions located nearby and within one large groove |
| Porencephaly Porencephalia (porencephalia, Greek: poros - passage, hole, pore + enliephalos - brain) is a pathological cystic expansion of the cerebral ventricle cavity of varying sizes, communicating with the subarachnoid space. In reality, the border between porencephaly and schizencephaly is blurred |
| Septo-optic dysplasia Septo-optic dysplasia - combined hypoplasia of the optic nerves and the absence or hypogenesis of the septum pellucidum, in 2/3 of cases accompanied by hypothalamic-pituitary dysfunction |
| Chiari malformation Chiari malformation is a congenital displacement of the structures of the posterior cranial fossa in the caudal direction |
Forecast
Long-term life prospects for people with schizencephaly vary depending on the size and location of the cleft and the degree of intellectual disability. For example, children with a small cleft in one hemisphere may have paralysis on one side of the body and have little or no intellectual disability, while clefts in both hemispheres can result in quadriplegia (paralysis of both arms and legs) and severe intellectual disability.
LABORATORY METHODS FOR STUDYING CHILDREN IN THE FIRST 3 YEARS OF LIFE IN A NEUROLOGICAL CLINIC
MORE: GO TO HOME PAGE