Pain
is an unpleasant sensation or emotional experience that occurs with the actual or potential threat of tissue damage or the term depicted by such damage (International Association for the Study of Pain, 1994). Pain is divided into acute and chronic.
· Acute pain
– this is a sensory reaction with the subsequent inclusion of emotional, motivational, vegetative and other factors that arise when the integrity of the body is violated. The duration of acute pain is determined by the recovery time of damaged tissue or impaired smooth muscle function. The main afferent highway is the neospinothalamic tract.
· Chronic pain
– pain that continues beyond normal healing, lasts for at least 3 months, is characterized by qualitatively different neurophysiological, psychophysiological and clinical relationships. Its formation depends to a large extent on a complex of psychophysiological factors and is often combined with depression.
Pain syndrome in the back and neck in various somatoneuro-orthopedic (vertebroneurological) diseases is the leading criterion for determining the severity of the patient’s condition, choosing therapeutic measures and conducting an expert assessment and labor prognosis. There are 4 degrees of pain in the back and neck:
Severe pain syndrome
– pain at rest, forced antalgic position, the patient cannot move, cannot sleep without taking sleeping pills and analgesics;
Severe pain syndrome
– pain at rest, but less, moves with difficulty within the room, an antalgic posture occurs when walking;
Moderate pain syndrome
– pain occurs only when moving;
Mild pain syndrome
– pain occurs only during heavy physical activity.
Objectification and assessment of the quantitative, qualitative and spatial characteristics of the pain phenomenon is carried out using special questionnaires.
Symptoms of tension
are associated with the occurrence of myofacial pain syndrome in the back and limbs in patients with degenerative-dystrophic diseases of the spine (Popelyansky Ya.Yu., 2003).
Previously accepted hypotheses about tension of the roots through herniated intervertebral discs during joint movement, liquorodynamic push, tension of the spinal cord and roots during neck flexion, etc. in patients with spinal osteochondrosis are currently only of historical interest, but the name of the symptoms remains the same.
1. Neri's symptom
– forced tilt of the head of a patient lying on his back leads to pain in the lumbar spine.
2. Symptom L
acera -
flexion of the legs in the hip joint in a patient lying on his back, leads to pain along the back of the thigh or in the lumbosacral region (phase 1). When the leg is bent at the knee joint, the pain disappears (phase II).
3. Sequart's sign
- flexion or extension of the foot of a patient lying on his back leads to pain in the popliteal fossa.
4. Bonnet's sign
- bringing the affected leg of the patient lying on his back causes pain in the lower back or along the back of the thigh.
5. Matskevich's symptom -
bending the leg at the knee joint in a patient lying on his stomach is characterized by the appearance of pain along the anterior surface of the thigh or in the groin fold.
6. Wasserman's sign
- raising the outstretched leg of a patient lying on his stomach causes pain in the lumbar region
Questions for self-control
1. Define comorbidity in neurology.
2. What does somatoneurology, neurosomatology, somatoneuroorthopedics study?
3. Give examples of somatoneurological comorbid disorders.
4. List standard trigger points for vertebroneurological diseases. Name the viscero-cutaneous projections.
5. Describe the normal range of motion in the spine.
6. Define acute and chronic pain.
7. Describe the severity of the pain syndrome.
8. Describe the methodology for studying Lasegue’s symptom.
9. Describe the method of studying the symptoms of Wasserman and Matskevich.
10. The patient has a positive Bonnet sign on the right; make a topical diagnosis.
Lasègue's symptom occurs against the background of tension in the roots of the sciatic nerve, which occurs due to pinching of the nerve fiber in the spine or spasmodic contraction of the lumbar and gluteal muscles. This and some other symptoms make up a group of “tension symptoms” - pain that occurs when nerve fibers are stretched.
Pain in the projection of damaged nerve fibers occurs when lifting the leg up while the person is lying on his back. The pathogenetic mechanism for the occurrence of the symptom is due to the fact that when the lower extremities move, the sciatic nerve has to stretch, but when it is pinched, the length of the nerve fiber decreases. Against this background, when the limbs are slowly lifted upward, the sciatic nerve is “overstretched,” which is why pain occurs.
Symptoms of tension
Symptoms of tension are signs of neurological diseases of the spine, which are accompanied by muscle spasms or other reasons that provoke difficulties in movement and stretching of the nerve roots.
The symptom of tension may indicate degenerative changes in the spine and osteochondrosis. Provoking passive movements causes acute pain. In neurology, there are 7 symptoms of tension:
- Dezherina;
- tripod;
- planting;
- Wasserman-Matskevich;
- Bonner;
- Neri;
- Lasega.
Positive Lasegue symptom. Symptoms of Lasegue, Neri in neurology :: SYL.ru
In medical practice, there are a huge number of different pathologies associated with impaired functionality of the spine. The causes of the disease may be different, but among them there are symptoms, the presence of which indicates pinched nerve fibers. One of these is the Neri symptom, the detection of which greatly facilitates diagnosis.
What it is?
When doctors use the term “tension syndrome in osteochondrosis,” they mean the appearance of pain symptoms that occur during passive movements of the arms and legs. The cause of these sensations is too much tension on the nerve roots that are located in the spinal cord. Tension also refers to spasms (sharp contractions) of muscle fibers.
The causes of such symptoms are pathogenic processes of destruction of vertebral bone tissue. As a result, they gradually shift and change location.
Therefore, the bones begin to compress the intervertebral discs, which is why they also collapse and have a mechanical effect on nerve fibers as well as muscle tissue. As a result, they become very stretched and cause significant pain to the patient.
This syndrome is a neurological manifestation of osteochondrosis, so first of all you should contact a neurologist.
Symptoms of tension intensify if, along with osteochondrosis, a person suffers from other chronic pathologies - ankylosing spondylitis, pinched sciatic nerve, hernia and protrusion of discs.
Lasègue test
The symptom was first discovered by the French neurologist Lasegue back in the mid-19th century. He conducted an experiment in which he discovered a sharp pain in a patient when raising a straight leg in a supine position; after bending the knee or hip joint, the painful sensations stopped instantly.
Pain when raising the lower limb in a straight position occurs due to stretching of the sciatic nerve, while the pain reaction can be caused by tension in only one nerve root. A painful reaction occurs due to compression of the nerve roots in the intervertebral foramen due to its excessive tension.
Normally, stretching of the nerve as part of a physiological process cannot cause its overstrain, and movement in the intervertebral foramen occurs smoothly, the root easily slides along it without excessive compression. Painful sensations may occur due to the fact that the nerve fibers of the sciatic nerve are not able to lengthen naturally, this may be due to pinching or overstretching.
The sciatic nerve is the largest nerve in the human body and positive Lasegue syndrome can indicate a number of diseases along its length. Doctors use the symptom of tension to make an accurate diagnosis of diseases of the lumbosacral spine.
Diseases that provoke the appearance of the syndrome
Diseases when the sciatic nerve becomes tense include:
Treatment of diseases that are accompanied by Lasègue's symptom consists of drug therapy with the use of painkillers, physiotherapeutic procedures, acupuncture, and the use of orthopedic corrective agents.
Therapeutic blockades with anesthetics help relieve pain, and after the patient’s condition has eased, manual therapy is used only on the recommendation of a doctor.
The identified positive result is the initial step in assessing the patient’s condition in a complex manner. It allows you to pay attention to the appearance of pathological processes in the body, determine the source of the lesion and begin its treatment.
How is the check carried out?
Testing for Lasegue's symptom can only be carried out by a neurologist.
Indications for the study may be patient complaints of discomfort in the lower back, gluteal muscles, thigh and lower leg muscles during movement. Discomfort may be manifested by limited movement, pain or numbness in the area of the sciatic nerve. It is possible that pain may appear on only one side, this indicates a unilateral lesion.
To carry out the procedure, the patient is placed on his back on a hard, stable surface. In the supine position, the patient does not experience any discomfort; the nerve roots are completely relaxed and do not cause pain.
The specialist slowly bends the limb at the hip joint, while the patient's knee should be bent. In this position, the nerve and its roots are still relaxed, and movement does not cause discomfort. Next, the doctor smoothly raises the leg, while the limb should be straight.
The Lasegue tension symptom is considered negative if the patient does not experience pain when lifting a straight limb. A symptom can be considered positive when the subject feels pain when raising the leg, and after bending the knee joint, the pain sharply disappears.
A false-positive symptom is most often observed in old people; it indicates weak muscle tone and is not associated with overstretching of the sciatic nerve.
Key points of the study:
- The limb should rise very smoothly; it is forbidden to bend the leg sharply, as this can cause serious damage to the sciatic nerve.
- The study should be stopped immediately after the onset of pain.
- The procedure cannot be performed on patients under the influence of painkillers or anesthesia. The result of such a study cannot be reliable, and the absence of a pain protective mechanism can cause rupture of nerve fibers.
- If a positive test for Lasegue's symptom is received, the patient must be referred for additional studies of the lumbosacral spine.
Diagnostic features
If the cause of the pathology is radiculitis, the patient exhibits Neri's symptom - a connection between head tilt and sensations in the lumbar region.
If the test result is positive, the person's pain should go away when they bend their knee.
Testing doesn't require much effort. Despite the simplicity of the examination, the patient’s reaction allows us to determine a number of parameters. During the procedure, several diagnostic features will be highlighted:
- The patient lies down on the couch. He lifts his leg independently or with the help of a doctor.
- If pain occurs at the level of 30°–40°, then the syndrome is positive. In this case, the pain should subside when bending the leg at the knee.
- Loss of sensitivity of the skin on the front surface of the thigh is allowed. This is a sign of osteochondrosis and compression of the 5th lumbar or 1st sacral nerve root.
- Pain that occurs at 70° indicates a pathology of muscle tissue and is not related to pinching of the sciatic nerve.
- If the pain does not subside after bending the leg, the test is called negative. The cause of discomfort in this case is joint disease.
During the examination the following rules must be followed:
- When lifting your leg, you should not bend it, as this will not allow the sciatic nerve to stretch.
- If the patient feels pain at 60°, the examination is stopped. Raising your leg even higher, despite the pain, increases the risk of nerve fiber rupture.
- All movements should be slow and smooth.
- The examination cannot be carried out if the patient has taken an anesthetic drug, as the result will be inaccurate.
- If Lasegue's symptom is detected, additional diagnostics are prescribed. An MRI is recommended to visualize the nerve fibers.
7823 0
Intervertebral discs
Intervertebral discs provide mobility to the spine, support it and distribute the load during movements. With age, the amount of proteoglycan in the disc core decreases, and the disc begins to dry out (loss of water). Mucoid degeneration and fibrous tissue ingrowth are observed, as well as ↓ disc space height and susceptibility to injury. Ring ruptures and nuclear protrusion occur as a result of intranuclear pressure under mechanical load.
Lumbar disc herniation
Clinical data
The posterior longitudinal ligament is strongest along the midline. The posterolateral portions of the annulus may be subject to greater stress. Therefore, most lumbar disc herniations (LDH) are observed posteriorly, somewhat to the side of the midline, compressing the nerve roots, causing characteristic radicular pain.
Various terms are used to describe the degree of disc protrusion based on sections or operating data: protrusion, sequestration, free fragment, etc.
Clinically, these differences are usually of little significance, the only difference being "limited prolapse" in which intradiscal interventions can be used. Characteristic data of the anamnesis:
1. complaints often begin with back pain, which after a few days or weeks gradually, and sometimes abruptly, turns into radicular pain with a decrease in back pain
2. it is rarely possible to identify factors that increase pain
3. pain decreases when bending the leg at the hip and knee
4. Patients usually avoid increased physical activity, however, prolonged stay in any position (sitting, standing or lying down) can increase pain, so a change in position is usually required every 10-20 minutes. This is in contrast to the severe pain observed, for example, with blockage of the ureter, when patients writhe from it
5. pain intensifies when coughing, sneezing or straining during defecation: in a series of observations66, a positive “cough shock symptom” was observed in 87% of cases
6. Urinary symptoms: The incidence of urinary disorders is 1-18%. In most cases, there is difficulty urinating or urinary retention. The earliest symptom may be decreased sensitivity of the bladder. Later, symptoms of “irritation” are often observed: increased urge, frequent urination (including nocturia), increased residual urine. Less common with radiculopathy are enuresis and urinary incontinence (note: true urinary retention may occur with cauda equina syndrome). Sometimes GPD may only present with urinary symptoms, which may improve after surgery. Laminectomy may improve bladder function, but this is not certain
Clinical manifestations of radiculopathy
Back pain as such is not a significant complaint (only 1% of patients with acute LBP have sciatica). If this is the only complaint, then other causes must be excluded. Sciatica is such a specific symptom of GPD that the likelihood of having clinically significant GPD in the absence of sciatica is only ≈1/1000. Exceptions are central hernias, which may cause symptoms of lumbar stenosis (eg, neurogenic claudication) or SCS.
Compression of the nerve root leads to certain symptoms of varying severity. For the most commonly involved roots, characteristic syndromes have been described.
In a series of patients referred to a neurosurgeon for pain radiating to the leg, motor impairment was present in 28% (although only 12% reported muscle weakness as a complaint), sensory impairment in 45%, and reflex impairment in 51%.
The following symptoms may indicate compression of the nerve roots. The sensitivity and specificity of some symptoms in patients with sciatica are given in Table. 11-8.
Table 11-8. Sensitivity and specificity of clinical findings of lumbar disc herniation in patients with sciatica
1. complaints and symptoms of radiculopathy (see Table 11-9) A. pain radiating down the leg B. muscle weakness C. sensory disturbances along the dermatomes D. reflex disorders: mental factors can influence the symmetry of reflexes
2. positive symptoms of nerve root tension: including Lassègue's sign
Table 11-9. Lumbar disc syndromes
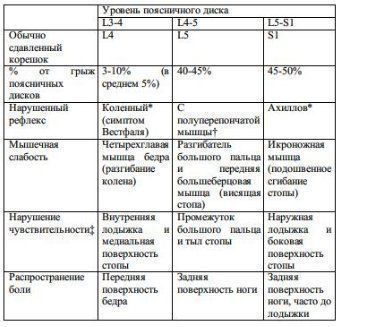
* the disturbance may be more noticeable when taking Jendrassik (during the test of the reflex, the patient pulls the clasped hands to the sides) † the reflex from the semimembranosus muscle is unreliable (it is not always only the L5 root), during testing the adductor muscles can also be stimulated ‡ sensory disturbances are more common observed along the lower border of the dermatome
Symptoms of nerve root tension
1. Lassegue's sign:
so-called straight leg raise test. Helps differentiate sciatica from hip pain. Methodology: the patient lies on his back, the sore leg is raised by the ankle joint until pain occurs (pain should appear at the angle
2. Crum test:
the patient lies on his back; lift the “sick” leg, slightly bending it at the knee, and then straighten it. The results are the same as when raising a straight leg
3. cross lift of a straight leg, so-called. Firestein test:
lifting the straightened “healthy” leg causes pain on the opposite side (this requires lifting to a greater angle than on the “sick” side). A more specific but less sensitive test than Lassegue's sign (97% of surgical patients who tested positive for this test had confirmed GPD). May correlate with a more central position of the hernia
4. hip stretch test or so-called. reverse straight leg raise test:
the patient lies on his stomach, the examiner's hand is on the popliteal fossa, the knee is maximally bent. The test is often positive for compression of the L2, L3 and L4 roots (ie, upper lumbar disc herniations) or for extremely lateral herniations (may also be positive for diabetic femoral neuropathy or psoas muscle hematoma). In these situations, the straight leg raise test (Lassegue's sign) is often negative (because the L5 and S1 roots are not involved)
5. bow string symptom:
After pain occurs when lifting your straightened leg, bend your knee and lower your foot onto the bed, continuing to keep your leg bent at the hip joint. With this maneuver, the pain caused by sciatica is relieved, but the pain in the hip joint remains
6. straightening the leg in a sitting position:
The patient is seated with both hips and knees flexed 90°. In this position, one knee is slowly extended. In this case, the same tension in the nerve roots occurs, as in moderate lifting of a straightened leg.
Other useful symptoms for radiculopathy
1. Patrick's test:
the ankle joint is placed on the knee of the other leg, and then the ipsilateral knee is moved towards the surface on which the patient is lying. This creates tension in the hip joint and usually does not increase true nerve root compression. The test is often positive in cases of hip involvement (eg, trochanteric bursitis) or mechanical LBP
2. Trendelenburg's sign:
the examiner looks at the pelvis from behind while the standing patient raises one leg. Normally, the pelvis should remain horizontal. If the symptom is positive, the pelvis tilts downwards on the side of the elevated leg, indicating weakness of the abductor muscles of the opposite thigh (main innervation of L5)
3. cross adductors:
When testing the knee reflex, the adductor muscles of the opposite thigh contract. With an increased ipsilateral knee reflex, this may indicate damage to the upper motor neuron (UMN), and with a decreased ipsilateral knee reflex, this may indicate pathological spread, indicating excitability of the nerve root
Nerve root syndromes
According to the data below, GPD usually does not affect the root emerging at the level of this space, but compresses the root that exits through the intervertebral foramen one level below (eg, L5-S1 GPD usually causes S1 radiculopathy). This leads to the formation of characteristic lumbar nerve root syndromes, shown in Table. 11-9.
Important anatomical facts about lumbar discs:
1. in the lumbar region, the nerve roots emerge below and close to the root of the arch corresponding to them by vertebral number
2. the intervertebral space is located below the level of the arch root
3. in the most typical structure of the human spine there are 24 presacral vertebrae, although in some cases there may be 23 or 25 A
. Therefore, the GPA of the last gap usually compresses the 25th nerve root (although, in accordance with the above individual characteristics, this may be the 24th or 26th root)
A
possible options: 11 or 13 vertebrae with ribs or lumbosacral transitional vertebra; the terms “S1 vertebral lumbarization” or “L5 vertebral sacralization” are imprecise and may be misleading
X-ray diagnostics
Conservative treatment
Surgery
Indications
Despite numerous attempts to determine which patients will improve on their own and which should be operated on more quickly, this has not yet been established.
1. ineffectiveness of conservative treatment: in more than 85% of patients with acute GPD, improvement will occur without surgery within an average of 6 weeks (in 70% within 4 weeks). Most experts recommend waiting about 5-8 weeks after the onset of radiculopathy before considering surgery (bearing in mind that there are no indications listed below)
2. “EMERGENCY INTERVENTION” (before 5-8 weeks have passed): indications: A. cauda equina syndrome (CAS) B. progressive movement disorders (eg foot drop): paresis of unknown duration is a questionable indication for surgery ( No studies have shown that patients in this situation have less severe motor deficits after surgery). However, acute onset or progression of movement disorders is considered an indication for urgent surgical decompression C. “emergency” surgery may be indicated for patients whose pain remains intolerable despite sufficient narcotic medications
3. ± patients who do not want to wait and try whether conservative treatment will help them, if there is still a question about surgery later
Greenberg. Neurosurgery
Lasègue's symptom occurs against the background of tension in the roots of the sciatic nerve, which occurs due to pinching of the nerve fiber in the spine or spasmodic contraction of the lumbar and gluteal muscles. This and some other symptoms make up a group of “tension symptoms” - pain that occurs when nerve fibers are stretched.
Pain in the projection of damaged nerve fibers occurs when lifting the leg up while the person is lying on his back. The pathogenetic mechanism for the occurrence of the symptom is due to the fact that when the lower extremities move, the sciatic nerve has to stretch, but when it is pinched, the length of the nerve fiber decreases. Against this background, when the limbs are slowly lifted upward, the sciatic nerve is “overstretched,” which is why pain occurs.
Causes of the syndrome
The main reason for a positive result when testing for Lasegue's sign is a herniated disc. The mechanism of occurrence of the symptom is due to the fact that the tissues supporting the intervertebral disc in their physiological position are damaged, stretched, and the disc can shift towards the spinal canal.
In the canal, the disc can put pressure on the roots of the sciatic nerve; in a relaxed state, the patient does not experience pain, but when tensioned, the nerve must go around the body of the intervertebral disc, this forces it to stretch to a greater length, but it is not capable of this. In this case, painful sensations occur in the lumbar region. Detection of such a symptom requires additional x-ray examination to clarify the diagnosis.
The appearance of pain during the test in the area of the gluteal muscles may indicate osteochondrosis of the lumbosacral region.
Diseases accompanied by Lasegue's symptom:
- osteochondrosis;
- neoplasms in the area of the sciatic nerve;
- the occurrence of intervertebral hernia and disc displacement;
- sciatic nerve damage;
- compression of the nerve root by muscles in the buttock area;
- compression of the distal spinal column;
- accumulation of mineral salts in the ligaments in the spine area.
When this happens
The Neri symptom is checked quite often in neurology. And here we are most often talking about certain diseases of the back or spine, among which it is worth noting:
- Myeloradiculopathy. Most often it develops in the lumbar region and leads to pinched roots in the L5-S1 area. Concomitant manifestations include loss of tendon reflexes, impaired sweating, loss of skin sensitivity, and the onset of changes in the lower extremities. A laboratory examination of the cerebrospinal fluid may reveal an increased content of red and white blood cells.
- Inflammation of the nerve roots, which is popularly called. This pathological condition occurs with osteochondrosis of the spine and is combined with intervertebral hernias, tumors, and injuries.
- Muscle spasm of the lower back muscles. This condition is diagnosed with hypothermia and the process can involve not only muscle tissue, but also the spinal nerves that pass through them. In this situation, the Neri test is positive because compression of the nerve fiber occurs.
- Grades 2–4 are formed when the height of the vertebrae is reduced by more than half.
When conducting the test, you should remember that each person has their own pain sensitivity threshold, so you cannot focus only on this symptom when making a diagnosis. Therefore, in each case, it should be understood that before making a diagnosis, it is necessary to listen to all the patient’s complaints, conduct other examinations, and only on the basis of this make the correct diagnosis and begin treatment.
Evaluation of the results obtained
The occurrence of pain when raising the leg at an angle of 60 degrees cannot indicate a positive Lasègue symptom; this is due to the fact that at this angle the nerve reaches its maximum stretch.
Bending the limb at an angle of 40-60 degrees also causes maximum stretching of the nerve; painful sensations may not be associated with a symptom of tension, but indicate that the length of the nerve has reached its limit.
Only bending the leg at an angle of up to 30 degrees indicates a true Lasègue symptom.
The manifestation of Lasegue's syndrome may indicate the development of certain diseases of the lower spine, but is not a prerequisite for establishing a final diagnosis. To accurately determine the disease, methods for identifying other symptoms of tension, fluoroscopy and MRI are used.
What diseases cause this symptom?
The dependence of painful sensations with Neri's symptom is a consequence of processes associated with damage to the spine and the formation of formations that are capable of one way or another putting pressure on the nerve endings.
Thus, a symptom may indicate the presence of:
- herniated intervertebral discs;
- tumor formations;
- developing osteochondrosis, within which pronounced bone growths are formed;
- vertebral displacements;
- protrusion of intervertebral discs;
- radiculitis of the lumbosacral spine.
It is worth noting that the intensity of painful sensations usually does not have a direct relationship with the degree of development of the problem. Each individual has a different sensitivity threshold, so the Neri symptom can be either strong or mild.
There are several options for the manifestation of a symptom depending on its cause:
- at the very beginning of the development of the disease, the pain syndrome can be extremely mild, which makes determining the Neri symptom and other symptoms of tension difficult. The further the disease progresses, the more obvious these manifestations become;
- when nerve roots are pinched, pain is almost always present, and the symptom is detected without any difficulty;
- with a lateral herniated disc, neurological symptoms are pronounced, and pain may be insignificant. In this case, the Neri symptom may not be observed until the disc protrusion reaches a size of 10 mm.
The Neri symptom is an important diagnostic tool that allows timely identification of a number of diseases of the spinal column. A specialist can assess its severity and can also create a list of possible problems. In combination with other symptoms of tension, the diagnosis becomes more accurate, which allows timely treatment of the identified problem and monitoring the dynamics of the pathological process.
The so-called “tension” and “position” symptoms are based on myofixation (reflex, subconscious) of the affected motor segment due to irritation of the receptors of its deformed tissues and causing an increase in intradiscal pressure in a number of symptoms. When conducting experiments on animal corpses, it was proven that nerves have a reserve of length and the ability to move in relation to adjacent tissues in the fascial bed, as a result of which there is practically no tension on the nerve.
Main symptoms of position and tension:
1. Fenz's symptom - the phenomenon of "oblique" rotation. If you rotate your head tilted forward in both directions and pain occurs, this indicates the presence of rubbing spondylotic growths of adjacent vertebrae. 2. Klein's symptom - with forced turns and tilting the head back, feelings of dizziness, nausea, and noise in the head may occur. This indicates the involvement of the vertebral artery in cervical osteochondrosis. 3. Spurling's symptom - the phenomenon of the “intervertebral foramen”. When a load is placed on the head, tilted on the shoulder or tilted and turned to the painful side, paresthesia or pain occurs, radiating to the innervation zone of the root, which is subject to compression in the intervertebral foramen. 4. Bertschi test - the patient sits on a chair, the doctor stands behind the patient and covers the lower jaw with his palms, presses his head to his chest, rises on his toes, as a result, the cervical spine is stretched (compression of the roots is relieved, blood flow through the vertebral arteries improves). If at the same time the nature and intensity of noise and pain in the neck, head or ear changes, this indicates the involvement of the cervical spine in the occurrence of cerebral symptoms. 5. Neri's symptom - with active and passive tilting of the head forward, pain occurs in the area of the affected root. 6. Symptom of “axial load” - when pressure is placed on the patient’s head along the vertical axis, pain and paresthesia in the area of the affected root increase. 7. Lhermitte's symptom - when the head is tilted sharply forward, pain occurs in the form of an electric current passing through the entire body along the spine. 8. Symptom of “raised and lowered arm” - a decrease in pain with a horizontal position of the arm and an increase with the addition of paresthesia at night with the lowered arm; allows you to differentiate the discogenic process from the infectious and toxic ones. 9. Symptom of “reins” - when the thoracic vertebrae are affected, the long muscles of the back below the level of the lesion are tense and when the patient bends over, they tense up in the form of tense reins. Usually the symptom is sharply positive in secondary radiculalgia (tuberculosis, metastasis, Schmorl's hernia). 10. Bonnet test - hip adduction is accompanied by tension in the piriformis muscle, and in the presence of neuroosteofibrosis, pain. 11. Lasègue’s symptom - there are three degrees of its severity:
I - mild: pain appears when raising the leg to an angle of 60°, not intense, there is a moderate protective contraction of the muscles of the back, abdominal wall, pelvis;
II - moderately severe: pain appears when raising the leg to an angle of 45°, a sharp protective contraction of individual muscles occurs, a moderate autonomic reaction;
III - pronounced: the angle of leg elevation is up to 30°, a generalized protective muscle contraction and a sharp autonomic reaction occur. There are modifications of Lasegue's symptom that can be used in expert cases: a) the appearance of pain when lowering the leg from the edge of the couch with the patient lying on his stomach; b) study of Lasegue’s symptom with the patient standing; c) Vengerov's maneuver: contraction of the abdominal muscles when examining Lasègue's symptom (it is necessary to first divert the patient's attention), etc. 12. Ankylosing spondylitis's symptom (crossed Lasègue's symptom) - the occurrence of pain in the “sick” leg when examining Lasègue’s symptom on the healthy side. 13. Symptom of “squatting” - bending of the affected leg or both legs when the patient tries to sit up in bed with straightened legs. 14. Waserman's symptom - the appearance of pain along the anterior surface of the thigh when lifting a straightened leg upward in a patient lying on his stomach. 15. Matskevich’s symptom is the appearance of pain along the anterior surface of the thigh when flexing the lower leg in a patient lying on his stomach. 16. Dejerine's symptom (“cough point”) - the appearance of pain in the lower back when coughing, sneezing, or straining. 17. Sicard's symptom - pain along the sciatic nerve with strong plantar flexion of the foot in a lying patient. 18. Govers-Sicard symptom - pain along the sciatic nerve with strong dorsiflexion of the foot. 19. Turin's symptom - pain along the sciatic nerve with strong dorsal extension of the thumb. 20. Razdolsky’s symptom (“bell”) - when pressing on the interspinous ligament, spinous process, paravertebral points, the pain radiates to the radicular or sclerotomal zone of the affected leg. 21. Symptom of a “locked back” - the patient develops a sensation of lumbago after attempting to lift a weight or at the moment of a sharp bend or extension of the body in the form of severe pain in the lower back or in the lumbosacral region, fixing the body in a bent position; patients cannot move, as any movement causes sharp pain. 22. Amos symptom - characterized by a peculiar transition from a lying position to a sitting position: when trying to sit down, the patient helps himself by resting his hands on the lumbar region. This symptom is noted in vertebrogenic lumbosacral pain syndrome. 23. Panov-Lobzin-Churilov marching test - in a standing position, the patient is asked to march in place, simultaneously palpating the lumbar paravertebral muscles. On the side of pain (homolateral side), pronounced muscle tension is detected.
Often, patients with vertebrogenic pathology also have autonomic disorders. Thus, trophic changes manifest themselves in the skin and subcutaneous tissue in the form of impaired sweating (anhidrosis or hyperhidrosis), peeling of the skin, wrinkling, thinning, swelling; in the form of pain at the points of attachment of muscles and tendons to bone protrusions.
A number of autonomic pain points are also palpated.
1) A. M. Grinstein point (orbital) - at the inner corner of the orbit. 2) Temporal artery point - palpated by sliding palpation. 3) Point of the vertebral artery - located medial to the posterior edge of the sternocleidomastoid muscle, below the occipital points on the line connecting the apex of the mastoid process and the spinous process of the epistrophy at the border of the outer and middle third. 4) The point of the superior cervical sympathetic ganglion is at the level of the C2-C7 vertebrae, medial to the supra-Derbian points on the anterolateral surface of the bodies. 5) Point of the stellate ganglion - from the transverse process of the C7 vertebra to the head of the first rib. 6) Points Markelov - Birbrair - carotid artery, superior trigeminal, phrenic nerve (above the middle of the clavicle), shoulder girdle (in the middle third), midpoint of the shoulder, radial artery, thenar, intercostal, vertebral (D-3), solar plexus (on the middle of the distance between the navel and the pubis), Lapinsky (at the inner edge of the popliteal fold), artery of the feet.
Vasomotor disorders are manifested by chilliness of the limbs, a pronounced venous pattern; decreased temperature of both or one foot, dorsum of the hand, forearm (Erben's symptom); decreased pulsation of the arteries of one or both feet, often on the side of more severe pain (Wartenberg's symptom).
There is an asymmetry in the color of the skin of the feet and hands. So, if the limb is pale and cold to the touch, then the arterioles suffer; if cyanotic, cold - then arteries and venules; if cyanotic, warm - then venules.
The easiest way to identify vegetative-vascular changes is the Bogolepov test. The patient stretches his arms forward - determine the color of the skin of the hands and blood flow. Then he raises one limb as high as possible, and lowers the other down. After 30 seconds, the patient raises his arms to the starting position. In healthy individuals, the color of the nails becomes the same after 30 seconds.
Patients with vertebral artery irritation syndrome experience a feeling of fog before the eyes, headache, paracusis, intolerance to noise and bright light, dizziness, nausea, palpitations, pain in the heart area (cervical migraine). The state of the tone of intracerebral vessels is judged by the state of the retinal arteries, by the sensations that arise when turning and tilting the head and during Bertschi traction.
Patients may experience a sensitivity disorder of sympathetic origin, mild hypoalgesia in the form of a half-hood or half-jacket. There may also be reflected visceral symptoms, especially from the urinary and gallbladder.
Attention is also paid to the presence of a direct Claude-Barnard-Horner symptom (constriction of the pupil, palpebral fissure and retraction of the eyeball) or reverse. The reaction to ultraviolet radiation changes (less on the pain side), the galvanic test, blood pressure, pulse, rheovasography, and kymography indicators change.
3435 0
For the first time, the symptom of pain in the lower back and sciatic nerve during bending of the straight leg in the area of the hip joint was described by the French doctor Lasegue.
The syndrome was then named after this physician.
To understand the essence of the syndrome, you should pay attention to the largest nerve in a person - the sciatic, which is formed by the roots of the nerves of the spinal cord.
If a traumatic effect or excessive tension on this nerve causes a sharp movement in a person lying on his back when they try to lift or bend the limb, then Lasegue tension syndrome manifests itself.
Treatment
As a rule, when treating any neurological disease, a comprehensive solution to the problem is necessary. This means that for effective therapy it is necessary to use not only medications, but also physiological procedures.
Drug therapy must necessarily include the use of non-steroidal anti-inflammatory drugs as an analgesic component. This includes drugs such as Diclofenac and Ibuprofen.
For more severe pain, the patient is advised to use Nimesulide, Dexketoprofen, Meloxicam, and so on. Dosages and treatment regimens are prescribed by the doctor individually for each patient and depend on the severity of symptoms.
Often the treatment regimen includes two steps:
- First, use the drug in injections to quickly relieve the problem.
- Maintaining well-being with oral medications.
Another medicinal component whose prescription is often mandatory is muscle relaxants. For example, “Mydocalm” is a drug based on tolperisone. The substance eliminates inflammation and damage to the nerve fiber. It comes in injection and tablet form.
It is useful to prescribe B vitamins to the patient. As a rule, the drug of choice in this case is “Compligam B” or “Kombilipen”. The drugs include vitamins B1, B6, B12 and lidocaine as an anesthetic component. With such a powerful composition, the medicine effectively nourishes the nervous system and supports its healthy functioning.
Wasserman-Matskevich symptom: possible causes, diagnostic methods and treatment
Neurological diseases are among the most common among the adult population. Many people are familiar with pain in the neck, shoulder blades, lower back or sacrum. All this is the result of excessive stress, incorrect posture, and complications of other diseases.
Any such pathology can lead to a deterioration in general well-being and the development of pain. Therefore, it is so important to promptly and correctly identify the cause of the ailment and begin to take measures to eliminate it.
Thus, one of the methods of early and reliable diagnosis is the procedure for determining Wassermann's symptom.