Amyotrophy neural Charcot-Marie (peroneal muscular atrophy) has a slow progression.
The disease is based on atrophy of muscle fibers in the distal parts of the legs.
It belongs to the category of diseases with a genetic predisposition. It is inherited mostly as an autosomal dominant trait and less frequently as an autosomal recessive trait.
Fiber degeneration occurs in peripheral nerves and their roots. There are cases of hypertrophic changes in interstitial tissue. The mutation in the muscles has a neurological basis. Individual muscle groups atrophy.
The later form of the disease is characterized by hyaline degeneration and complete breakdown of muscle fibers.
Often the disease is accompanied by significant changes in the spinal cord . The area of the anterior horns is affected, as well as the lumbar and cervical spine, which disrupts nerve conduction in the spinal cord.
This condition is characteristic of hereditary Friedreich's ataxia.
Characteristic
Neural amyotrophy, also known as Charcot-Marie-Tooth disease, is a genetic disease that causes weakening and thinning of the lower leg muscles. Atrophic changes in muscle tissue lead to a decrease in muscle volume in the lower extremities.
Charcot-Marie-Tooth disease is characterized by damage to the nerve endings that transmit information from somatosensory receptors to parts of the brain. At the same time, damage occurs to the neuronal motor pathways through which signals are transmitted from the cortical control centers to the executive organs - skeletal muscles.
Charcot-Marie-Tooth disease is inherited (usually in an autosomal dominant manner) and is considered as a neuropathy (nerve dysfunction) of the sensory-motor type. The onset of the disease can occur in early childhood or later in life. The prevalence of the pathology is 1 case per 2500 people.
The autosomal dominant type of inheritance suggests that a single defective gene that is passed on to the child becomes the cause of the development of the pathology. In the ICD-10 list, Charcot-Marie-Tooth disease is listed under code “G60” (motor-sensory neuropathy of hereditary origin).
Kinds
The forms of the disease are distinguished taking into account the nature of damage to nerve endings belonging to the peripheral nervous system. Type 1 pathology develops due to demyelination - destruction of the myelin sheath covering the nerves. Normally, the myelin sheath improves the transmission of nerve impulses. It debuts more often in middle childhood (4-5 years), less often in adolescence.
The first symptoms: weakness in the feet, atrophic changes in the muscles of the distal legs. Atrophic changes in the muscle tissue of the hands develop later. Along with the loss of sensitivity (inability to distinguish temperature, perceive painful stimuli, vibration), a decrease (sometimes loss) of tendon reflexes is observed in the area of the hands and feet.
Charcot-Marie-Tooth polyneuropathy type 2 develops against the background of damage to axons - the branches of neurons through which communication is carried out between individual elements of the neuronal network. This is a slowly progressive form. Onset symptoms may appear in older children. During instrumental diagnostics, relatively normal indicators of the speed of nerve impulses are revealed.
In parallel, a decrease in the difference between the amplitude values of action potentials (excitation wave) of sensitive nerve cells is observed. Another feature is polyphasic (multiphasic) action potentials in the region of muscle fibers. A biopsy shows Wallerian-type axonal degeneration, the process of destruction of a section of an axon.
Causes
Genetic aspects and classification. Types and genes: • type 1A: 118220, PMP22, CMT1A, 601097 (myelin protein 22), 17p11.2; • type 1B: 118200, MPZ, CMT1B, 159440, 1q22; • type 2A: CMT2A, 118210, 1p36 p35; • type 2B: CMT2B, 600882, 3q13 q22; • type 2D: CMT2D, 601472, 7p14; • type 4A: CMT4A, 214400, 8q13 q21.1; • type 4B: CMT4B, 601382, 11q23; • X linked 1, dominant: 302800, GJB1, CMTX1, 304040 (connexin gene CX32, Xq13.1); • X linked 2, recessive: CMTX2, 302801, Xp22.2; • demyelinating: CMTND, 601596, 5q23 q33; • with skin aplasia (302803) • with palmoplantar keratoderma and nail dystrophy (148360) • Couchok's syndrome (310490) • with Friedreich's ataxia (302900) • with deafness (118300, 214370) • with tremor (214380) • with ptosis and parkinsonism (118301)
Pathomorphology • Hereditary sensorimotor neuropathy type I - histologically segmental demyelination and remyelination, concentric growth of Schwann cells (hypertrophic neuropathy) • Hereditary sensorimotor neuropathy type II - histologically Waller's degeneration.
Causes and pathogenesis
The main reason for the development of type 1 peroneal atrophy is duplication (the appearance of an additional copy of a chromosome section) of the PMP22 gene (17th chromosome) of the myelin protein in the sheath of peripheral nerves. The pathogenesis of Charcot-Marie-Tooth disease involves damage to motor nerve endings, which is accompanied by dysregulation of muscle contraction.
The pathogenesis involves the process of damage to sensory nerve endings, which leads to a disruption in the transmission of information from somatic sensitivity receptors in the peripheral parts of the body to the corresponding centers of the brain. Neural amyotrophy reflects degenerative, atrophic changes in peripheral nerve fibers and, less commonly, in the spinal cord.
Treatment approach
Treatment is carried out in accordance with the existing symptoms of neural amyotrophy of Charcot Marie Tooth. The activities are comprehensive and lifelong.
It should be noted that more effective treatment methods are not known to medicine. Only methods are used that help alleviate the patient’s condition and improve their quality of life.
It is important to optimize the patient's functional coordination and mobility. Treatment measures should be aimed at protecting weakened muscles from injury and decreased sensitivity.
The patient's relatives should help him in every possible way in the fight against this disease. After all, treatment is carried out not only in medical institutions, but also at home.
All prescribed procedures must be followed strictly and carried out daily. Otherwise, there will be no results from the treatment.
Treatment of amyotrophy includes a number of techniques:
- physiotherapeutic procedures;
- occupational therapy;
- a set of physical exercises;
- special support devices for the feet;
- orthopedic instep supports to correct deformed feet;
- feet care;
- regular consultation with your doctor;
- the use of orthopedic surgery;
- injections of B vitamins;
- prescription of vitamins E, A, C.
Additionally use:
- For amyotrophic lesions, a specific diet is prepared . It is recommended to eat foods with high protein content; patients adhere to a potassium diet and should consume more vitamins.
- If the course of the disease is regressive, in parallel with the above remedies, mud, radon, pine, sulfide and hydrogen sulfide baths are prescribed . An electrophoresis procedure is used to stimulate the peripheral nerves.
- If there is impaired mobility in the joints and skeletal deformation, correction by an orthopedist is indicated .
To alleviate the emotional state of the patient, psychotherapeutic conversations are required.
The basis of treatment is the use of agents that help improve trophic indicators and the transmission of impulses along nerve fibers.
Drug treatment
For this purpose, the use of medications such as:
- glutamic acid;
- aminalon;
- dibazole;
- biostimulators of anabolic hormones;
- often resort to the use of adenosine triphosphoric acid, cocarboxylase, cerebrolysin, riboxin, phosphaden, carnitine chloride, metnonine, leucine;
- good results are achieved by means that optimize blood microcirculation: nicotinic acid, xanthinol nicotinate, nikoshpan, pentoxifylline, parmidine;
- To improve conductivity in nerves, anticholinesterase drugs are prescribed: galantamine, oxazil, pyridostigmine bromide, stephaglabrine sulfate, amiridine.
Symptoms
The first symptom of Marie-Charcot-Tooth is muscle weakness in the area of the foot and lower leg (the part of the leg from the knee joint to the heel). Muscle weakness is accompanied by a change in the ability to perceive external stimuli. The patient loses the ability to sense external temperature, vibration, and pain. The progression of the disease is accompanied by the spread of sensory loss to the proximal (located closer to the center of the body) segments of the limbs.
The clinical picture varies significantly. In some patients, the pathology is asymptomatic, in others, during a diagnostic examination, a decrease in the speed of nerve impulses in muscle tissue is revealed, in others there is a significant limitation in motor activity associated with muscle atrophy and weakness. Symptoms typical of Charcot-Marie-Tooth disease:
- Atrophic changes in the muscles of the extremities, mainly in the tissue of the peroneal and distal (distant from the center, end) muscles. Due to atrophy of the muscle tissue of the lower leg, the lower limbs resemble the legs of a stork or an upside-down champagne bottle.
- Muscle weakness in the affected leg segments. The patient experiences difficulty bending the leg at the ankle joint to elevate the distal segment of the foot.
- Muscle weakness in the affected arm segments. The latest symptom that indicates the progression of the pathology.
With a mild course, isolated signs may be observed, for example, a peculiar shape of the toes that resemble a hammer, or a high instep of the foot. Typically, symptoms are more severe in men. Women often have no symptoms. Charcot-Marie-Tooth syndrome in the initial stages may include symptoms: acute painful sensations in the muscles, paresthesia (spontaneously occurring feeling of burning, tingling, crawling). Other signs of CMT in children and adults:
- Foot drop. Photos of patients clearly show that the forefoot droops due to weakening of the muscles when the leg is elevated. The patient cannot independently lift the forefoot segment higher.
- Gait disturbance, which is characterized as shuffling and slow. When walking, the patient touches the surface on which he walks with his toe. To prevent shuffling on the surface, patients are forced to raise their legs high when walking.
- Dangling foot with a significant spread of atrophic processes.
- Friedreich's foot (recession of the interdigital spaces, high arch, hammer-shaped toes).
Charcot-Marie-Tooth syndrome includes symptoms: decreased sensitivity in the distal segments of the limbs, muscle cramps in the forearms and calf muscles. A typical sign of late stages (10-15 years after the manifestation of the disease) is impaired fine motor skills of the hands, which is accompanied by dysfunction of writing.
The patient cannot hold a handle or fasten or unfasten buttons on clothing. Vegetative-trophic disorders in the form of hyperemia (redness of the skin) and increased sweating in the area of the hands and feet are less common. Patients are often diagnosed with fractures of the bones of the foot and sprains of ligaments and tendons in the ankle area.
哈尔滨楠木南中医门诊部
Hereditary neuropathy Charcot-Marie-Tooth (CMT) is the most common from hereditary polyneuropathies. In the article there is a review of Russian and foreign investigations in the field of non-pharmacologic methods of treatment in the recent 10 years.
Here there are up-to-date principles of physiotherapeutic treatment with the use of natural and preformational physical factors, adapted physical exercises and recommendations for sanatorium treatment. For the first time the authors modified the standards of non-pharmacologic treatment of CMT patients, considering the time history and the type of the disease, the electromiographic data of the initial autonomic patient`s status. Key words: hereditary neuropathy (CMT), non-pharmacologic treatment, hereditary neuro-muscular diseases, physiotherapy, massage, adapted physical exercises.
Neural amyotrophy of Charcot-Marie-Tooth is a progressive chronic hereditary disease with damage to the peripheral nervous system, leading to muscle atrophy of the distal legs and then the arms. Along with atrophy, hypoesthesia and extinction of tendon reflexes, fascicular muscle twitching are observed. Diagnostic measures include electromyography, electroneurography, genetic counseling and DNA diagnostics, nerve and muscle biopsy. Treatment is symptomatic - courses of vitamin therapy, anticholinesterase, metabolic, antioxidant and microcirculatory therapy, exercise therapy, massage, physiotherapy and hydrotherapy.
Hereditary neuropathy Charcot Marie Tooth
Abstract: Charcot–Marie–Tooth hereditary neuropathy (CHMT) is the most common form of hereditary polyneuropathies. This article provides an overview of available domestic and foreign developments in the field of non-drug methods of treating NNSCT over the past 10 years. Modern principles of physiotherapeutic treatment using natural and preformed physical factors, organization of therapeutic physical education classes, and recommendations for sanatorium-resort treatment are presented. For the first time, the authors modified the standards of non-drug treatment of patients with NNSCT, taking into account the severity, type of disease, electromyographic data, and the patient’s initial vegetative status.
Epidemiology.
The prevalence of NNSCT in the Russian Federation varies from 7.14 to 13.3 per 100,000 population in different regions and accounts for about 80% of all hereditary neuropathies.
Differences in epidemiological data are due to the heterogeneity of this disease. This means that the clinical form of the disease can be caused by mutations at different loci or multiple alleles at a single locus. The genetic heterogeneity of NNSCT determines the clinical polymorphism of this disease in carriers of mutations of the same gene, explains the different types of inheritance, and the features of electroneuromyographic changes.
Classification of NNSHM.
Currently, taking into account neurological and histopathological studies, two main forms of the disease are distinguished: demyelinating (CMT1) and axonal (CMT2). An intermediate form with signs of both CMT1 and CMT2, a spinal form of CMT with involvement of the spinal cord in the pathological process, are also known.
Type 1 NSCT accounts for about 70% of clinical cases of the disease. The X-linked form of the disease accounts for about 10-20% of all cases of NCC. Currently, more than 25 loci have been identified, and more than 30 genes have been identified that cause NNSMT. Data on the characteristics of the course of various types of NNSCT make it possible to determine treatment tactics.
NNSCT affects all races and nationalities without age or gender differences, but people of young, working age (20-30 years old) are more often affected. Despite significant advances in the study of the molecular genetic mechanisms of hereditary neuromuscular diseases, the identified specific mutant genes and their proteins, the progressive course of the disease with the development of disabling motor complications and the lack of effective treatment in patients with NNSCT leads to a significant decrease in the quality of life.
Complaints.
The main complaint presented by patients is paroxysmal pain such as short-term cramps in the calf muscles (the so-called “cramps”), which intensifies after prolonged physical activity at night; difficulties in walking and increasing deformities of the feet, which most limit motor capabilities. Some patients experience sensory deficits in the arms and legs in the form of loss of pain sensitivity, numbness, burning, tingling, or complain of so-called “gouty” pain in the ankle joints and chronic fatigue.
Clinic.
The disease begins with damage to the distal extremities.
Symptoms of the disease usually develop in the second decade of life (12-15 years), however, there are forms with an early onset (6-7 years). The earlier the disease manifests itself, the more severe it is. There are forms with early onset at the age of 3-5 years, which are accompanied by lesions of the bronchopulmonary system, auditory and visual analyzer, intestines, and bladder.
Upon examination, symmetrical hypotrophy of the muscles of the dorsal surface of the feet, peroneal muscles, and deformities of the feet are revealed: an increase in the arch with a hammertoe deformity of the toes of both feet (“Friedreich’s foot”). As a result of damage to the extensors and abductors, the foot hangs down, and the patient develops a characteristic gait - stepping. The lower leg muscles are involved in the process in the later stages of the disease. Sharply thinned shins with well-preserved thigh muscles give the leg the characteristic appearance of the legs of a stork or an overturned bottle. Achilles reflexes are usually reduced or absent, while more proximal reflexes remain intact. Usually, after 5-10 years from the onset of the disease, the small muscles of the hands, as well as the muscles of the forearm, begin to atrophy, as a result of which the hand takes on the shape of a monkey’s paw. Due to the weakness of the muscles of the hands, mainly the flexors, some patients may need various devices to improve everyday adaptation - “bottle openers”, buttons on clothes instead of buttons, turn signals for door handles and other aids[4-7]. In severe cases of hand deformity, orthosis is indicated. Life expectancy and intelligence are not affected by NNSCT.
A common complication of NSCT is ankle sprains, ankle sprains and fractures. To support foot drop and improve the support functions of the lower extremities, patients with cervical spine injuries need additional orthopedic products: orthoses for the ankle and knee joints, and posture correctors for those with scoliotic deformity.
In some patients with the onset of NCC in early childhood, changes in the bronchopulmonary system are common: weakness of the chest muscles that provide expiratory pressure, which complicates the course of diseases accompanied by cough and congestion in the lungs.
It should be noted that with NNSCT of any type, peripheral nerves are primarily affected, and muscle damage is secondary. In the later stages of cervical cancer, muscle tissue breaks down (rhabdomyolysis) and is replaced by fibrous and fatty fibers.
Rehabilitation and habilitation
Rehabilitation is a dynamic system of interconnected medical, psychological and social components (in the form of certain influences or activities) aimed not only at restoring health, but also at the possible complete restoration (preservation) of the personal or social status of a sick or disabled person [11]. From the standpoint of the above, the term “rehabilitation” is valid in cases where the object is a person who is ill for the first time, and the effect of rehabilitation involves the full or partial restoration of impaired body functions, a return to professional activity and the integration of a seriously ill or disabled person into society.
Habilitation is (from Latin abilitatio; from Latin Habilis - comfortable, adaptive) - therapeutic and/or social measures in relation to disabled people or people with disabilities, aimed at their adaptation to everyday or professional life.
Due to the hereditary nature of the disease, its steady progression, the impossibility of a complete cure and restoration of lost functions, the goal of therapy for NNSCT is to slow down the progression and adapt patients to everyday life. In connection with the above, it is most appropriate to use the term “habilitation” for patients with NNSCT. The beginning of the process of habilitation of patients with NNSCT depends on the form of the disease and should begin from the moment of early clinical manifestations, and in cases where this is possible, in the absence of symptoms of the disease, from the moment of genetically confirmed diagnosis. Already at the preclinical stage of NNSCT, it is possible to use physical factors and exercise therapy in order to delay the onset of clinical manifestations of the disease. The process of habilitation of patients with NNSCT should continue throughout the entire period of the patient’s life.
Until now, there is no clear understanding of the role of non-pharmacological methods in the treatment and habilitation of patients with NNSCT and their scientifically substantiated use in this pathology.
The presence of a large selection of physical factors makes it possible to select and adjust therapeutic interventions for any patient with NCC.
The goal of non-drug treatment is to: slow down the development of degenerative muscle degeneration; improving regional blood circulation, increasing muscle strength; performance and reserve capabilities of muscles; reducing the risk of injury (dislocations, sprains, fractures), joint diseases with subsequent development of contractures; normalization of the patient's vegetative status.
In determining the tactics of non-drug treatment of NNSCT, EMG data helps to determine the predominant type of peripheral nerve damage (axonal, demyelinating, mixed) and the patient’s vegetative status.
Currently, non-drug treatment methods for NNSMT include: physiotherapy, balneotherapy, therapeutic massage (manual and instrumental), therapeutic physical education, orthopedic treatment, manual therapy, acupressure, reflexology, diet therapy, cultural and vocal therapy. In accordance with the objectives of habilitation of NNSMT, physiotherapy includes the following factors: factors that improve the metabolism of nervous and muscle tissue; trophostimulating methods; factors that improve regional lymph and blood flow, microcirculation; factors that improve neuromuscular conduction; factors that normalize the functions of the central and autonomic nervous system.
The use of medicinal electrophoresis of metabolic stimulants helps to enhance metabolism, enhance the reparative processes of nervous and muscle tissues, improve the conduction of impulses along the nerve, accelerate the regeneration of damaged nerves, increase the ATP content in tissues, and improve tissue respiration. Native mud preparations (peat, biosed, humisol), vitamins B1, B6] are used as drugs that improve the metabolism of neuromuscular tissue.
For non-drug treatment of NNSMT, all types of therapeutic mud are used in the form of mud applications or galvanic mud. Expected effects of peloid therapy: slowing down the processes of destruction of the myelin sheath of nerves, stimulating remyelination, as a result - improving nerve conduction; stimulation of axonal growth, reduction and prevention of the development of contractures due to the thermal factor.
In order to improve neuromuscular conduction in patients with the axonal form of NNSCT, electrophoresis of anticholinesterase drugs (prozerin, galantamine, neuromedin) is used.
Ukrainian researchers have obtained data on the effectiveness of neuromidin as a drug that helps improve neuromuscular conduction and increase muscle contractility. The drug helps to slow down the development of the pathological process in neuromuscular diseases, including NNSCT.
In cases of osteoporosis, it is advisable to prescribe calcium electrophoresis to the segmental zones of the spine, phosphorus electrophoresis to the dorsum of the hands and feet.
To improve tissue trophism in NNSCT, a number of authors recommend the use of low-frequency magnetic therapy with diadynamic currents and amplipulse therapy. When using low-frequency electrotherapy, blood circulation and various types of metabolic processes in the affected muscles increase, the RNA content in muscle tissue increases, and conditions are created to prevent the development of atrophic processes. Under the influence of low-frequency magnetic therapy, the catabolism of glucose and lipids is activated, the course of intracellular biochemical reactions is accelerated, peripheral circulation and transcapillary filtration are enhanced, and the restoration of damaged peripheral nerves is accelerated. It has been proven that a magnetic field increases the mobility of the axoplasm of nerve fibers. This promotes the formation of growth flasks and activates the transport of protein complexes from the bodies of nerve cells to the periphery along the lines of force, causing the directed growth of conductors. Magnetic therapy reduces the severity of pain and vegetative-vascular disorders in the distal limbs. The therapeutic effect of magnetic therapy is more pronounced in the area of damaged structures.
Electrical stimulation of paretic muscles has found widespread use for the treatment of motor disorders in patients with cervical spinal cord injury, both in domestic and foreign practice. Under the influence of electrical stimulation, the metabolism of muscle tissue is activated, which helps restore the conductivity and excitability of peripheral nerves and accelerate their regeneration. The trophism of nerve conductors increases, muscle strength increases, and their tolerance to physical activity increases. Electrical stimulation is carried out according to the classical method, depending on electromyography or electrodiagnostic data.
Darsonvalization of the limbs and segmental zones is used as a method that irritates free nerve endings, activates axon growth, and gently corrects the vegetative manifestations of NNSCT.
In the treatment of muscle wasting and atrophy, and the presence of pain syndrome, interference currents are applied to segmental areas of the spine and limbs. Under the influence of interference currents, the electrical excitability and bioelectrical activity of muscles increases, peripheral blood circulation and tissue trophism improve, as a result of which pain decreases, mobility in joints increases while being limited by degenerative-dystrophic processes[. A feature of interference therapy is its good tolerability, which allows its use in elderly people.
To enhance reparative and regenerative processes in nervous tissue, a number of authors recommend the use of ultrasound. It is known that at a sonication dose of 1 W/cm2, the cytoplasm of cells undergoes rapid circular motion, which intensifies physiological processes in the cell, and this in turn leads to a positive biological effect. In nervous tissue, this phenomenon manifests itself in changes in the content of mucopolysaccharides, the structure of myelin sheaths and the acceleration of myelination of growing axons.
In the later stages of NNSCT, the formation of deformities and contractures of the joints of the hands and feet is characteristic. To treat contractures in combination with exercise therapy, paraffin or ozokerite applications are used on the affected joints, as well as high “gloves” and “stockings”, however, the temperature regime should be taken into account due to the presence of pain and temperature sensitivity disorders.
If there are changes in the bronchopulmonary system, Ukrainian authors have proposed a method of singlet oxygen therapy (valkion therapy). The mechanism of action of singlet oxygen therapy is based on photochemical sensitization of air or water using a halogen lamp with the formation of secondary singlet oxygen, which carries an additional charge of energy, enhancing phosphorylic respiration of mitochondria. Valkion therapy helps activate tissue metabolism at the cellular level, reduce tissue hypoxia, promote regeneration of the bronchial mucosa, and improve their drainage function. Valkion - therapy is used in combination with breathing exercises, gentle manual techniques, electrical stimulation of the back muscles. The following scheme is used on the Valkion device from Poly-Valk (Sweden): 1st day - 100 ml of water, 5 min of inhalation; 2-3 days - 150 ml of water, 9 minutes of inhalation; 4th and subsequent days - 200 ml of water, 14 minutes of inhalation. Course No. 15, 3-4 courses per year.
Valkion therapy is used in combination with a drinking solution of Stimol according to the following scheme: children aged 2-5 years - 100 mg (1/2 sachet) 2 times a day, 5-12 years - 200 mg (1 sachet) 2 times/day, over 12 years old - 200 mg (1 sachet) 3 times/day. within 30 days in courses (every 3 months).
It is recommended to carry out physical treatment systematically, for a long time, alternating courses every 2-3 months.
There are rehabilitation treatment programs using complex therapy (medication, physiotherapy, kinesiotherapy, orthopedic treatment) for patients with hereditary neuromuscular diseases. Analysis of long-term results (5 years or more) indicates that complex treatment can stabilize the condition of many patients with NNM for a significant period of time (from one to several years), and in some cases even improves muscle activity and leads to an increase in quality of life patients.
Physiotherapy
The goals of physical therapy: maintaining and increasing muscle strength, normalizing walking function, minimizing injuries, stretching tense and spasming muscles, supporting and improving the functional state of the cardiovascular system.
The main part of the physical training program for patients with NSCT with motor disorders and pain syndrome is stretching exercises for spasmed and shortened muscles (arch of the foot, calf muscle, hamstrings and Achilles tendons). A number of American authors believe that the combination of stretching and wearing braces leads to a significant reduction in the progression of contractures of the lower extremities.
The next group of exercises are strengthening exercises using weights, resistance, and gymnastic apparatus (balls, gymnastic sticks, tourniquets, weights). In some patients, exercise can help slow the rate of loss of muscle strength, while in others it can significantly increase it. American research supports the idea that even neurologically damaged muscles can be strengthened. Maximal strength training is not recommended for patients with NCCMT, which can lead to the depletion of initially reduced muscle reserves, as well as the breakdown of muscle tissue. Excessive weights and overwork lead to injuries to healthy muscles. At the same time, when training damaged muscles, the number of loads and repetitions that are traumatic will be reduced by the patient himself due to the initial weakness of the muscles. Injury to an already weakened muscle jeopardizes its continued performance.
Due to the presence of sensory ataxia in patients with NSCMT, coordination exercises using gymnastic apparatus and stabilizing platforms are required to be included in the training program.
In order to activate general motor skills in children with motor deficits and disorders of simple movements, running, jumping and climbing on a gymnastic wall are used. In the general physical training program, special attention is paid to aerobic exercises to train the cardiorespiratory system: cycling, swimming, race walking.
Running is not recommended for such patients due to the high probability of injury to the joints and ligaments, especially the ankles. Race walking is 80% of the effectiveness of jogging and is considered the most acceptable and safe for such patients. Due to the danger of injury and worsening the course of the disease, anaerobic strength training is strictly prohibited for patients with cervical cancer without prior consultation with a rehabilitation specialist. An initial consultation with patients with NCC is carried out to determine the strength and degree of preservation of certain muscle groups, the presence of concomitant diseases, and the degree of physical fitness using various tests. Based on the data obtained, the neurologist-rehabilitation specialist develops an individual physical training program with which the patient can exercise independently, including in the gym. Patients can perform a strengthening complex at home, subject to periodic visits to a neurologist-rehabilitator so that he can adjust the set of exercises depending on the dynamics of the patient’s condition. It should be noted that patients with NSCT due to foot deformities often experience certain difficulties and need the correct selection of shoes both for everyday life and for training.
Massage
In domestic and foreign practice of habilitation of patients with NSCT, therapeutic massage has found wide use in order to improve the trophism of muscle tissue, reduce cramps, and improve blood and lymph flow. Russian authors( ) recommend the following technique: selective massage, primarily for the muscles of the lower extremities using techniques for relaxing the triceps muscles and finger flexors and stimulating massage for the extensors of the feet and fingers. General massage of all parts of the body - stroking, rubbing, kneading techniques, excluding percussive techniques.
A number of authors recommend the use of massage only of intact muscles using a gentle technique due to the risk of aggravating degenerative processes in the affected muscles.
Orthotics
Due to the characteristic syndrome of progressive muscle weakness and hypotrophy, accompanied by tendon retraction in conditions of predominance of the functions of the most intact muscles, in patients with cervical cervical cord injury, the biomechanics of the step are disrupted with the development of persistent contractures and limitation of motor functions. For most forms of cervical spine injury, damage to the musculoskeletal system begins with the formation of equino-varus, equino-valgus feet, and foot drop. Weakness of the peroneal and calf muscles, frequent falls, gait disturbances, prevention of musculoskeletal deformities and fractures are indications for wearing orthoses. For CMT, two types of orthoses are used: auxiliary and corrective. Joint orthoses perform the following functions: fixation of the feet in a given position, correction of the arch of the foot. These orthoses are worn at night and provide long-lasting and gentle stretching. Used more often in children. In addition, orthoses redistribute the load evenly over the entire lower limb and reduce the load on the distal parts of the lower limbs. Most often, orthoses perform several functions simultaneously. Clinical observations show that effective correction is achieved through daily (at least 3 months) use of orthoses. Orthosis is one of the means of complex treatment and habilitation of patients with NNSCT]. As NNSCT progresses, scoliotic deformities, hyperlordosis of the lumbar spine, hyperkyphosis of the thoracic spine and flexion contractures of the joints of the hands may occur, which is not only a neurological problem, but also an orthopedic one.
Surgical treatment
During the surgical treatment of patients with hereditary neuromuscular diseases, the following tasks are solved: improving the supporting function of the foot in independently moving patients in order to prolong the ability to walk; facilitating the care and everyday adaptation of patients with severe contractures of the ankle and wrist joints, in particular, and with severe pain; preventing the development or increase of respiratory failure in severe deformities of the chest and spine;
As a rule, operations are performed at the final stage of treatment for severe forms of cervical cancer.
Spa treatment
Sanatorium-resort treatment is carried out for patients with preventive, therapeutic and habilitation purposes, for patients with the initial and advanced stages of the disease. The purpose of sanatorium-resort treatment is to prevent the progression of the process, correct vegetative status, increase the functional and compensatory capabilities of the body. Preference should be given to balneological and mud resorts located in identical climatic conditions that do not require heavy adaptation. Preference is given to balneological resorts with chloride, radon, hydrogen sulfide springs, and mud resorts.
Currently, the team of authors of this article, in accordance with the pathogenesis, features of the clinical course of NNSCT, data from paraclinical studies, is developing the most effective complexes of non-drug treatment for NNSCT, including physiotherapy, massage, and physical therapy.
Attachments:
· ·
·
Diagnostics
Diagnosis is made based on clinical data and history. More often, similar cases are mentioned in the family history. The main instrumental method for diagnosing Charcot-Marie-Tooth disease is electromyography (the study of the conductivity of bioelectric impulses by muscle structures). Diagnostic criteria:
- Muscle weakness in the distal arms and legs.
- Early onset of the disease (in childhood, adolescence). If the pathology debuts in infancy, it is characterized by a severe course, which often leads to disability.
- The presence of similar symptoms in close relatives.
- Presence of deformities in the toes and instep of the foot.
- Sometimes there is pain when palpating the neurovascular bundles.
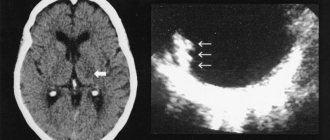
The diagnosis can be confirmed by the result of a genetic analysis, which indicates the presence of a chromosomal mutation. Neuroimaging (MRI, CT) reveals areas of demyelination (remyelination) in the area of peripheral nerves. Based on the results of the diagnostic examination, the doctor prescribes treatment for Charcot-Marie-Tooth disease.
Treatment
Charcot Marie Tooth disease is treated based on developed clinical guidelines. There are no methods of etiotropic (aimed at eliminating the causes of the disease) therapy. Treatment of Charcot Marie Tooth disease is palliative in nature, aimed at stopping symptoms and improving the patient’s quality of life. Treatment cannot stop the progression of neural amyotrophy.
However, the use of orthoses (medical devices designed to change the structural and functional characteristics of the neuromuscular system), physiotherapy, occupational therapy and psychotherapy help improve the patient’s social adaptation and quality of life. Patients typically wear splints to support foot drop.
Sometimes surgery is performed to stabilize the foot. Treatment of Charcot-Marie-Tooth pathology involves regular, dosed physical activity and massage, including classic manual, hardware and acupressure. Therapeutic exercises help reduce muscle weakness and maintain motor activity.
Charcot-Marie-Tooth disease is hereditary, like von Willebrand-Diane disease (a hereditary blood pathology characterized by the occurrence of spontaneous bleeding like hemophilia); in order to effectively treat it, complex measures are prescribed, such as drug therapy, physiotherapy, balneotherapy (therapeutic showers and baths), mud therapy.
To improve the trophism (nutrition) of muscle and nervous tissue and stimulate metabolic processes, drugs are prescribed: Cocarboxylase, ATP, Riboxin (participates in the metabolism of purine nucleotides necessary for normal muscle contractions), Cerebrolysin (has a nootropic effect), Methionine (regulates lipid metabolism).
To improve blood microcirculation, the drugs Pentoxifylline and Nicotinic acid are indicated. Correction of impulse conduction in muscle tissue is carried out using the drug Proserin (cholinesterase inhibitor). A comprehensive program of drug treatment includes taking vitamins B, A, C, E.
To prevent foot deformation, wear comfortable shoes that do not squeeze the foot and do not restrict movement. Gait disturbances are corrected with braces such as AFOs (ankle-footorthoses). Such devices help control the flexion of the legs and ankle joint and ensure balance.
The use of orthoses is associated with long-term physical activity, prevention of falls and injuries, and the ability to self-care. Orthoses support the foot in a physiological position. Patients who regularly wear orthoses move independently and do not require assistance.
Treatment of Charcot-Marie-Tooth disease
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist. Dosed exercise therapy and massage, orthopedic measures, vitamin preparations, neurotrophic agents that improve microcirculation, and anticholinesterase drugs are indicated.
Essential drugs
There are contraindications. Specialist consultation is required.
- Sodium adenosine triphosphate (an agent that improves metabolism and energy supply to tissues). Dosage regimen: intramuscularly, in the first 2-3 days, 1 ml of a 1% solution is administered once a day, in subsequent days, 2 times a day or immediately 2 ml of a 1% solution once a day. For a course of treatment - 30-40 injections.
- Pentoxifylline (an agent that improves microcirculation). Dosage regimen: orally, swallowing whole, during or immediately after a meal, with plenty of water, at a dose of 100 mg 3 times a day, followed by a slow increase in dose to 200 mg 2-3 times a day.
- Milgamma (B complex of vitamins). Dosage regimen: therapy begins with 2 ml intramuscularly 1 time per day for 5-10 days. Maintenance therapy - 2 ml IM two or three times a week.
- Methandrostenolone (anabolic steroid). Dosage regimen: orally, before meals in a dose of 0.005-0.01 g 1-2 times a day. The course of treatment in adults lasts 4-8 weeks. Breaks between courses are 4-8 weeks.
- Cerebrolysin (nootropic drug). Dosage regimen: used parenterally in the form of intramuscular injections (up to 5 ml) and intravenous injections (up to 10 ml). The drug in a dose of 10 ml to 50 ml is recommended to be administered only through slow intravenous infusions after dilution with standard solutions for infusion. The duration of infusions ranges from 15 to 60 minutes. Administered parenterally in a dose of 5 ml to 30 ml/day. The recommended optimal course of treatment is daily injections for 10-20 days.
- Galantamine (anticholinesterase agent). Dosage regimen: orally, the daily dose for adults is 10-40 mg in 2-4 doses.