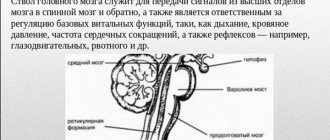
The brain stem is one of the important parts of the human central nervous system, since its sections contain nerve centers responsible for the regulation of all vital processes in the body, as well as the nuclei of the oculomotor and other cranial nerves, the function of which is to control the muscles of the face. For this reason, even minor damage to the brain stem by various neoplasms threatens the patient with disorders in the functioning of internal organs.

Types of lesions
Most often, brain stem tumors are diagnosed in children in the first years of life and in adolescence, with the peak incidence usually occurring at 4-6 years of a child’s life. Most of these neoplasms histologically represent gliomas of various formations:
- Astrocytomas. Occurs in more than 50% of clinical cases. It develops as a result of tumor damage to glial tissue cells - astrocytes, which perform a protective and auxiliary function in relation to neurons. Depending on the structural structure, all astrocytomas are divided into 2 categories: malignant and benign tumors. The former include pilocytic and fibrillar neoplasms, and the latter include anaplastic and multiform neoplasms.
- Ependymomas. They are rare, but they cause hydrocephalus and increased intracranial pressure even in the early stages of development.
- Oligodendrogliomas. They can reach large sizes, while the neoplasm has clear boundaries and does not grow together with the surrounding tissues.
- Glioblastoma. It is an aggressive type of glial malignant tumor.
According to the nature of their location in the tissues of the trunk, glial tumors are of 2 types:
- Expansive neoplasms. They have a clear location and do not merge with surrounding structures. Thanks to this feature, they can be easily removed surgically, after which in half of the cases the patient recovers completely.
- Infiltrative neoplasms. These include diffuse glioma of the brain stem, which, on the contrary, does not have a clear location, and its cells grow into the surrounding tissues and displace them, which is why the affected part ceases to function properly. Due to the fact that such a tumor cannot be removed without affecting the functional parts, the prognosis of the disease in most cases is unfavorable.
Brain stem - structure and functions
20.03.2019
The brain stem is a collection of structures of the central nervous system with a length of 7 centimeters, located between the spinal cord and diencephalon.
In the anatomical literature there are sometimes discrepancies : sometimes the diencephalon and cerebellum itself are included in the trunk.
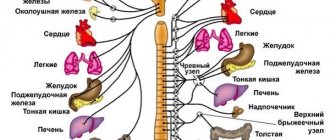
This set of sections contains the nuclei of the cranial nerves, which are responsible for maintaining life at the physiological level (respiratory processes, heartbeat centers, defecation and urination). The trunk is the most ancient formation in human evolution.
The sequence of locations of the brain stem sections is as follows (from top to bottom):
- Midbrain.
- Pons.
- Medulla.
Topographically, the brain stem begins from the slope of the base of the skull to the foramen magnum, located on the occipital bone. This formation is the largest information collector: the structures of the trunk regulate the flow of neural impulses between the telencephalon cortex and the formations of the spinal cord.
In addition to the large parts of the central nervous system, the brain stem also includes:
- red core;
- reticular formation;
- nervous structures of the tegmentum of the quadrigeminal;
- black substance.
Functions
The brain stem is responsible for the following simple and complex functions.
The simple include :
- Contraction of the oculomotor muscles and the muscle that lifts the upper eyelid.
- Change in pupil size (accommodation and constriction).
- Movement of the lower jaw, contraction of the masticatory muscles and tension of the eardrum.
- Receiving sensitive information from mucous membranes and skin. Data about temperature and pain in different parts of the body passes through the trunk.
- Contraction of facial muscles; contraction of the muscle located in the middle ear (regulation of sound flow).
- Regulation of the exocrine glands: sublingual, lacrimal, salivary.
- Control of body posture and balance.
- Innervation of the muscles of the pharynx and larynx - swallowing processes.
Complex include :
- A complete act of chewing, which includes regulation of the muscles of the tongue, jaw movement, salivation, and sensitivity of the oral mucosa.
- Reflex chain of the act of swallowing: root of the tongue – muscles of the soft palate – pharynx – esophagus.
- Vomiting reflex. It occurs when the mucous membrane of the tongue root, stomach, esophagus, and some parts of the intestinal tract are irritated.
- Cough reflexes. The mucous membrane of the larynx, trachea or bronchi perceives the stimulus and sends information about it to the brain stem. This, in turn, sends impulses to the respiratory center, which triggers a complex act of coughing with a strict sequence: deep inhalation - muscle contraction - narrowing of the bronchi (pressure in the lungs increases) - sharp and strong exhalation with instant opening of the gap.
- Sneeze reflexes.
- Functions of the reticular formation. The reticular formation of the brain stem regulates the tone of some flexor and extensor muscles of the trunk. This structure is also responsible for both activation and inhibition of the cerebral cortex (wakefulness-sleep cycle). In addition, the Russian Federation takes part in the functions of breathing, changes in vascular tone, sneezing, swallowing and coughing.
- Antinociceptive function. Its essence lies in the fact that the structure of the brain stem produces neurohormones, the action of which is associated with the suppression of the feeling of pain. This function is activated in a number of cases when a person experiences severe pain: labor, fractures with dislocations, phantom pain.
Descending Paths
Descending projection pathways are a group of tracts that send neural information from the telencephalon cortex and subcortical formations to brainstem structures. These include:
- Pyramid path. This tract connects the motor gyrus with the motor nuclei of the brainstem. So, with the help of this path, a person manages to control the muscles of the neck, head, eyes, face and torso.
- Extrapyramidal pathway. Thanks to this tract, people maintain their balance in space.
Research methods
Diagnosis of the functional state and activity of the trunk is carried out using clinical and instrumental laboratory methods. The first includes:
- neurological study of the activity of cranial nerves;
- study of voluntary movements;
- diagnostics of coordination of limbs and body;
- sensitivity study;
- Laboratory methods include:
- spinal puncture and examination of cerebrospinal fluid;
- X-ray of the skull;
- ventriculography;
- pneumoencephalography;
- Dopplerography;
- electroencephalography;
- magnetic resonance imaging;
- computed tomography.
Pathologies and diseases
The many manifestations of brain stem damage are due to the huge number of functions of this part of the nervous system. Most often, diseases are associated with deviations in sleep rhythms, disturbances in oculomotor activity, and lack of regulation of muscle tone. In order to correctly understand the clinical picture, the signs should be divided into groups, depending on the section of the trunk.
https://www.youtube.com/watch?v=c8dvuyulHck
Pathology of the midbrain :
- Weber's syndrome. This pathology is manifested by impaired coordination of the eye muscles, weakening of the muscle strength of the tongue and face, squint, drooping upper eyelid and bifurcation of objects.
- Akinetic-rigid syndrome is a pathological increase in muscle tone in combination with slow movements.
Bridge diseases include a complex of alternating syndromes:
- Bulbar alternating syndromes: dysfunction of the tongue muscles, various twitches.
- Pontine alternating syndromes: facial asymmetry, weakness of facial muscles, disruption of the oculomotor nerves.
- Peduncular syndromes: damage to the constriction and dilation of the pupil, protrusion of the eye from the orbit, partial or complete strabismus, paralysis and paresis of the facial muscles.
- Central hemiparesis: hypertonicity of the muscles of the hands and feet, pathological reflexes.
Disorders of the medulla oblongata :
- Impairment of all types of sensitivity on the skin of the lower extremities.
- Pathological drooping of the eyelid, constant constriction of the pupil, sunken eyes, pathological lack of sweat on the skin of the face.
A global pathology includes herniation of the brain stem (dislocation syndrome). This is a gross brain lesion, characterized by displacement of parts of the brainstem in relation to other parts of the brain.
In this condition, all vital centers that regulate the processes of breathing and heartbeat are disrupted.
The clinical picture includes impaired consciousness, respiratory failure, apnea (complete or temporary cessation of breathing), no swallowing, bulbar syndromes develop, and blood pressure drops rapidly.
The main treatment method is surgery. Doctors perform decompression craniotomy, an operation associated with reducing intracranial pressure. At the same time, specialists perform a puncture of the cerebrospinal fluid for the same purposes.
Didn't find a suitable answer? Find a doctor and ask him a question!
Source: https://sortmozg.com/structure/ctvol-golovnogo-mozga-stroenie-i-funktsii
Specifics of the disease
Due to the fact that the sections of the trunk contain nuclei of the regulatory formation, which are responsible for performing a large number of functional tasks of the human central nervous system, their damage by neoplasms is manifested primarily by the appearance of deviations in the functioning of certain internal organs, which significantly complicates diagnosis.
Initially, damage to the brain stem is manifested by the appearance of characteristic neurological abnormalities, for example, it may be a hearing disorder or uncontrollable twitching of the facial muscles. Further, as the tumor grows, the symptoms will intensify, headache and increased intracranial pressure will appear, which indicates the development of edema of healthy tissues.
As the situation worsens, the patient, to one degree or another, develops a syndrome of damage to the medulla oblongata, which is expressed in disruption of the functioning of internal organs and the development of central hemiplegia on the side of the body opposite to the tumor. For these reasons, when the first signs of damage to the trunk appear, the patient should seek medical help as soon as possible.
As practice shows, in a quarter of patients, the brain stem tumor is a benign neoplasm that can be removed surgically. At the same time, the remaining diffusely developing neoplasms are usually treated with radiation therapy.
Main symptoms
A glial tumor of the brain stem leads to organic damage to brain tissue, displacement of sections, and also causes circulatory problems in the organ, which causes symptoms characteristic of this disease:
- Headache. The appearance of this sign of damage to the brain substance is observed in 90% of clinical cases and is caused by an increase in the pressure of the neoplasm on the cranial nerves and blood vessels. Dizziness, darkening of the eyes, tinnitus and other manifestations of oxygen deprivation may also be present.
- Nausea, vomiting. Usually occurs during a headache attack and does not depend on food intake.
- Psychological deviations. It is observed in 65% of patients and manifests itself in changes in consciousness, irritability and apathy towards others.
- The patient experiences deterioration in clarity of vision, disordered pupillary reactions, loss of the inner halves of the visual fields, and paralysis of the facial muscles.
- The development of bulbar syndrome, which is characterized by the appearance of disturbances in the functioning of the functional centers of the medulla oblongata, that is, the patient has dysgraphia, aphonia, anarthria with impaired swallowing and articulation. Further, other manifestations of brainstem lesions arise: impaired cardiac activity, decreased blood pressure and the appearance of peripheral paralysis of the tongue muscles.
Also a distinctive feature of brain stem damage is an increase in the amount of cerebrospinal fluid in the subarachnoid space and, accordingly, an increase in the volume of the head.
Physiology of the brain
Topic 14
Physiology of the brain
Part
I. _
Brain stem Brain stem
- This is a part of the brain that includes the medulla oblongata, pons and midbrain. Here are the nuclei of the cranial nerves, structures of the reticular formation, nuclear formations related to the implementation of a wide range of reflex reactions of somatic and autonomic support of the higher functions of the central nervous system. In addition, ascending and descending pathways pass through the trunk, connecting it with the spinal cord and cerebral cortex. The brainstem loses the property of metamerism that characterizes the spinal cord and becomes a system of specialized nuclear formations. Physiologists include complex chain reflexes, regulation of tone and posture, and the influence of the reticular formation as stem functions.
► Functions of the brain stem, which are realized by the nuclei of the cranial nerves
.
The brain stem contains the nuclei of the III – XII pairs of cranial nerves, through which sensitive (sensory), motor (somatic) and vegetative (parasympathetic) functions are carried out.
╠ Nuclei of the oculomotor nerve
(III pair) are located in the midbrain.
The motor nucleus
contracts the superior, inferior, internal rectus, inferior oblique and levator palpebral muscles, participating in oculomotor reflexes.
Accessory (parasympathetic) nucleus
, innervating the sphincter of the pupil and the ciliary muscle, carries out the reflexes of constriction and accommodation of the eye.
╠ The nucleus of the trochlear nerve
( IV pair)
is located in the midbrain. Innervating the superior oblique muscle, it rotates the eyeball downwards and outwards.
╠ Trigeminal nerve
(V pair) has motor and sensory nuclei.
The motor nucleus
is located in the bridge, innervates the masticatory muscles and causes the movement of the lower jaw up, down, sideways and forward, and also strains the soft palate and eardrum.
Sensitive nuclei
(midcerebral, pontine, spinal) receive tactile, temperature, visceral, proprioceptive and pain impulses from the skin, mucous membranes, organs of the face and head. In addition, they are part of the conductive section of the corresponding analyzers and are involved in various reflexes, for example, chewing, swallowing, and sneezing.
╠ Abducens nerve nucleus
(VI pair) located in the bridge. Causes the eye to rotate outward by contracting the external rectus muscle of the eye.
╠ Nuclei of the facial nerve
(VII pair) are in the bridge.
The motor core
causes contraction of facial and auxiliary muscles, regulates the transmission of sound vibrations in the middle ear as a result of contraction of the stapedius muscle.
Sensory nucleus of the solitary tract
, innervating the taste buds of the anterior 2/3 of the tongue, analyzes taste sensitivity, participates in motor and secretory digestive reflexes.
The superior salivary (parasympathetic) nucleus
stimulates the secretion of the sublingual, submandibular salivary glands and lacrimal glands.
╠ Sensitive nuclei of the vestibulocochlear nerve
(VIII pair) are located in the medulla oblongata.
Vestibular nuclei
, innervating the receptors of the vestibular apparatus, participate in the regulation of body posture and balance (static and statokinetic reflexes), in the vestibulo-ocular and vestibulo-vegetative reflexes, and are included in the conduction section of the vestibular analyzer.
The cochlear nuclei
, which innervate the auditory receptors, participate in the auditory orientation reflex and are part of the conduction section of the auditory analyzer.
╠ Nuclei of the glossopharyngeal nerve
(IX pair) are located in the medulla oblongata.
The dual (motor) nucleus
causes the pharynx and larynx to rise and the soft palate and epiglottis to lower in the swallowing reflex.
The sensitive nucleus of the solitary tract
receives taste, tactile, temperature, pain and interoceptive sensitivity from the mucous membrane of the pharynx, the posterior third of the tongue, the tympanic cavity and the carotid body, is part of the corresponding analyzers, participates in the reflexes of chewing, swallowing, secretory and motor digestive reflexes, as well as in vascular and cardiac reflexes (from the caritid body).
The inferior salivary (parasympathetic) nucleus
stimulates the secretion of the parotid salivary gland.
╠ Nuclei of the vagus nerve
(X pair) are located in the medulla oblongata.
Double (motor) nucleus
, contracting the muscles of the palate, pharynx, upper part of the esophagus and larynx, is involved in the reflexes of swallowing, vomiting, sneezing, coughing, and in the formation of the voice.
The sensitive nucleus of the solitary tract, innervating the mucous membrane of the palate, root of the tongue, respiratory tract, aortic body, organs of the neck, thoracic and abdominal cavities, participates as an afferent link in swallowing, chewing, respiratory, and visceral reflexes. It is part of the conduction department of the interoceptive, gustatory, tactile, temperature and pain analyzers. Posterior (parasympathetic) nucleus
, innervating the heart, smooth muscles and glands of the neck, chest and abdominal cavities, is involved in cardiac, pulmonary, bronchial and digestive reflexes.
Get full text
╠ Motor nucleus of the accessory nerve
(XI pair) is located in the medulla oblongata and spinal cord and sends impulses to the sternocleidomastoid and trapezius muscles, which leads to their contraction and causes the head to tilt to one side with the face turned in the opposite direction, lifting the shoulder girdle up, and bringing the shoulder blades toward the spine.
╠ Motor nucleus of the hypoglossal nerve
(XII pair) is located in the medulla oblongata. Innervates the muscles of the tongue, causing its movement in the reflexes of chewing, sucking, swallowing and speech.
Thus, with the participation of the nuclei of the cranial nerves, the sensory and reflex (somatic and autonomic) functions of the brain stem are realized.
► Complex brainstem reflexes
. With the participation of the brain stem, complex somatic reflexes are carried out, each of which involves the nuclei of several cranial nerves.
1. Oculomotor reflexes
have centers that functionally unite the sensory nuclei of the trigeminal, vestibulocochlear nerves, tubercles of the quadrigeminal, motor nuclei of the oculomotor, trochlear and abducens nerves. Coordination of their activities is carried out by the reticular formation of the brain stem, as well as the cerebellum and cerebral cortex. As a result of these reflexes, friendly eye movements occur in different directions.
2. Reflex act of chewing
is provided by muscles that cause movements of the lower jaw and hold food between the dentition. Afferent impulses arise from various receptors of the oral mucosa and proprioceptors of the masticatory apparatus and spread mainly along the sensory fibers of the trigeminal nerve. The chewing center (the central generator of the chewing rhythm) is located in the reticular formation of the medulla oblongata and the pons and causes rhythmic excitation of the motor neurons of the muscles that raise and lower the lower jaw. The chewing rhythm generator can also be launched from the masticatory area of the frontal cortex, which provides voluntary control of chewing. The efferent influence of the chewing center is carried out through the motor nuclei of the V, VII and XII nerves.
3. Reflex act of swallowing
ensures the passage of food from the mouth to the stomach. When a bolus of food moves from the oral cavity to the esophagus, sequential stimulation of the receptors of the root of the tongue, soft palate, pharynx and esophagus occurs. The impulse through the sensory fibers of the trigeminal, glossopharyngeal and vagus nerves enters the swallowing center, which is located in the medulla oblongata and the pons. This center functionally unites neurons of approximately two dozen nuclei of the brainstem, cervical and thoracic segments of the spinal cord. As a result, a strictly coordinated sequence of contraction of the muscles that are involved in the act of swallowing is ensured: the muscles of the soft palate, pharynx, larynx and epiglottis, and esophagus. The swallowing center is functionally connected with the breathing center, which stops during each swallowing act.
4. Vomiting reflex
is a protective reaction that occurs when receptors in the root of the tongue, pharynx, stomach, intestines, peritoneum, and vestibular apparatus are irritated. Afferent impulses along the fibers of the glossopharyngeal, vagus or vestibulocochlear nerves enter the vomiting center located in the medulla oblongata. Vomiting can also be caused by direct irritation of the vomiting center by a local pathological process or chemicals. Efferent impulses from the vomiting center travel along the vagus nerve to the esophagus, stomach, intestines and through the spinal motor centers to the diaphragm and the muscles of the abdominal wall, the contraction of which leads to the movement of stomach contents.
5. Cough reflex
is a protective reflex that occurs when the receptors of the larynx, trachea and bronchi are irritated. Impulse along the sensory fibers of the vagus nerve excites the cough center of the medulla oblongata, which has efferent output to the spinal motor centers of the respiratory muscles. The cough center triggers a hard-coded sequence of reactions, in which three phases can be distinguished: 1) deep breath; 2) contraction of the expiratory muscles against the background of a closed glottis and narrowing of the bronchi, which leads to a sharp increase in pressure in the lungs; 3) active exhalation against the backdrop of instant opening of the glottis, creating a powerful air flow directed through the tension of the soft palate through the mouth.
6. Sneeze reflex
occurs when the receptors of the predominantly maxillary and partially ophthalmic branches of the trigeminal nerve are irritated in the mucous membrane of the nasal cavity, especially the middle turbinate and septum. The sneezing center, located in the medulla oblongata, organizes the same central systems as when coughing, but the flow of air during forced exhalation against the background of rapid opening of the glottis and lowering of the soft palate is directed primarily through the nose.
► Reticular formation of the brainstem
. The reticular formation is formed by a set of neurons located in the central parts of the brain stem, both diffusely and in the form of nuclei. Neurons of the reticular formation have long, poorly branched dendrites and a well-branched axon. These are multimodal neurons that have large receptive fields. In neurons of the reticular formation, the duration of the latent period consists of the sum of the latent periods of numerous synapses. RF neurons receive impulses from sensory pathways coming from different receptors and are highly sensitive to adrenaline, carbon dioxide, aminazine and barbiturates.
The reticular formation has connections with numerous structures of the central nervous system: ▓ Afferent inputs
enter the reticular formation from three sources: 1) from temperature and pain receptors along the fibers of the spinoreticular tract and the trigeminal nerve; 2) from the sensory and partly from other zones of the cerebral cortex, along the corticoreticular pathways, impulses enter the nuclei of the reticulospinal tracts and the nuclei that project to the cerebellum; 3) from the cerebellar nuclei along the cerebelloreticular pathway.
▓ Efferent outputs
from the reticular formation they are projected into the spinal cord along the lateral and medial reticulospinal tracts; 2) ascending pathways go to the upper parts of the brain (nonspecific nuclei of the thalamus, posterior hypothalamus, striatum), which begin in the nuclei of the medulla oblongata and pons; 3) there are pathways to the cerebellum that begin in the lateral and paramedial reticular nuclei and in the pontine tegmental nucleus.
Fig.1. Reticular formation of the brainstem. Scheme of the main afferent and efferent connections.
The variety of connections and structures of the Russian Federation determines its numerous functions, which can be combined into three main groups: somatic (motor), sensory (ascending influence on the cerebrum) and autonomic.
▓ Somatic functions of the Russian Federation
are manifested in its coordinating influence on the motor nuclei of the cranial nerves, spinal motor centers and the activity of muscle receptors.
▒ The reticular formation of the midbrain and medulla oblongata coordinates the functions of the nuclei of the oculomotor nerves (III, IV, VI), providing cooperative eye movements in the horizontal and vertical directions. With bilateral damage to these parts of the Russian Federation, voluntary horizontal and vertical eye movements become impossible.
▒ RF affects spinal motor centers (descending influence):
From the reticular giant cell nucleus of the medulla oblongata comes the lateral reticulospinal tract, the fibers of which end on the interneurons of the spinal cord. Through these interneurons, these fibers excite the ά- and γ-motoneurons of the flexor muscles of the limbs and reciprocally inhibit the extensor muscles. From the reticular nuclei of the pons comes the medial reticulospinal tract, which ends on the interneurons of the spinal cord. Through them, stimulation of ά- and γ-motoneurons of the extensor muscles of the trunk and proximal limbs is carried out. The flexors are inhibited through inhibitory interneurons.
▓ Sensory functions of the Russian Federation
. The ascending influence of the reticular formation on the cerebrum can be both activating and inhibitory. The impulses of the reticular neurons of the medulla oblongata, pons and midbrain arrive at the nonspecific nuclei of the thalamus, and, after switching to them, are projected to various areas of the cortex. In addition to the thalamus, ascending impulses also enter the posterior hypothalamus, striatum and septum pellucidum. The most important function of the ascending RF is the regulation of the sleep-wake cycle and the level of consciousness.
▓ Vegetative functions of the Russian Federation
. The reticular formation maintains the tone of the autonomic centers, integrates sympathetic and parasympathetic influences to realize the needs of the whole organism, transmits a modulating influence from the hypothalamus and cerebellum to the organs, being the most important structure of the vital centers of the medulla oblongata - cardiovascular and motor.
▒ Cardiovascular Center
represented by neurons that have access to the sympathetic and parasympathetic centers that innervate the heart and vascular tone. Therefore, the original name of this center was vasomotor, but is now being replaced by cardiovascular. The center scheme, proposed in 1946 by R. Alexander, consists of pressor and depressor zones.
Pressor zone
The vasomotor center is located at the level and above the lower angle of the rhomboid fossa in the posterolateral parts of the medulla oblongata. Its irritation leads to an increase in blood pressure and heart rate.
Depressor zone
The center is located at the level of the lower angle of the rhomboid fossa in the anterior parts of the medulla oblongata and the pons.
The pressor and depressor zones of the vasomotor center are not clearly defined anatomically and functionally: each of them contains both pressor and depressor points.
▒ Respiratory center
.
The respiratory center is a collection of neurons located at various levels of the central nervous system. The main part of the center is located in the medulla oblongata in the lower corner of the rhomboid fossa and consists of two symmetrical groups of neurons: dorsal and ventral. In addition to the medulla oblongata, the reticular formation of the pons also contains two groups of neurons involved in the regulation of breathing. One is located in the upper part of the bridge and is called the pneumotaxic center
, the second group is located in the middle and lower parts of the bridge and is called
the apneustic center
. The respiratory process also involves motor neurons of the spinal cord, which receive impulses from the neurons of the medulla oblongata and send them to the respiratory muscles along the phrenic and intercostal nerves.
► Brainstem reflexes
. Brainstem reflexes are triggered from receptors of the vestibular apparatus, proprioceptors of the neck, retinal receptors and tactile receptors.
▓ Regulation of muscle tone
. Efferent influences from the motor centers of the trunk spread to the muscles of the limbs and trunk along four descending pathways: vestibulospinal, rubrospinal, lateral and medial reticulospinal.
▒ Vestibulospinal tract
begins predominantly from the vestibular lateral nucleus, which receives afferent impulses from the receptors of the otolith apparatus and the ampullae of the semicircular canals.
Its fibers have an exciting effect on spinal ά- and γ-motoneurons of the extensor muscles of the limbs, trunk, and neck, as well as an inhibitory reciprocal effect on flexor motor neurons. The axons of neurons of the medial reticulospinal tract have the same effect .
▒ Rubrospinal tract
has the opposite effect on muscle tone.
This pathway begins from the red nucleus of the midbrain tegmentum and goes to the spinal cord, excitating the ά- and γ-motoneurons of the flexor muscles and reciprocally inhibiting the motor neurons of the extensor muscles. of the lateral reticulospinal
and pyramidal corticospinal tract have a similar effect on muscle tone
Thus, in the brain stem there are four main paired motor centers and pathways that regulate the tone of the muscles of the trunk and limbs.
▓ Setting reflexes
. Through the stem motor centers of the vestibulospinal, rubrospinal, medial and lateral reticulospinal tracts, the body's position in space is regulated, aimed at maintaining normal body posture and balance. The Dutch physiologist R. Magnus divided all adjustment reflexes into two groups: static and statokinetic.
▒ Static reflexes
determine the position of the body and its balance at rest. Magnus divided them into postural reflexes (body position) and righting reflexes.
╠ Posture reflexes
occur when the position of the head changes (a shift in the center of gravity) and is aimed at maintaining a normal posture. Afferent impulses come from the receptors of the otolith apparatus and proprioceptors of the neck muscles. Postural reflexes are divided into cervical and vestibular.
1. Neck reflexes
. The neutral position of the neck is the position in line with the body, while the impulse from the cervical proprioceptors is minimal. If the neck deviates dorsally, a reflex extension of the upper limbs occurs. If the neck is tilted ventrally, then reflex extension of the lower extremities occurs. When the neck tilts to the side, the extensors on the side of the tilt are activated.
2 .
Vestibular reflexes
. Afferent impulses come from the labyrinth of the inner ear.
When a person is in a vertical position
there is an increase in the tone of the extensor muscles of the lower extremities and flexors of the upper extremities. At the same time, the cervical and labyrinthine reflexes reinforce each other.
╠
Rectifying reflexes
are a more complex version of static reflexes, thanks to which the body is able to return to a natural position after its violation. Reflexes are carried out from the receptors of the cervical muscles, labyrinth, skin, and retina, with the obligatory participation of the midbrain. Important components of these reflexes are the cervical, vestibular and optical righting reflexes, and the first motor reaction is the restoration of the normal position of the head. Next, a chain of reflex reactions occurs with a redistribution of muscle tone in the limbs and torso, as a result of which normal body posture is restored.
Get full text
▒ Statokinetic reflexes
occur during acceleration of linear and rotational motion of the body. In this case, muscle contractions are aimed at overcoming the accelerations acting on a person, maintaining normal posture, balance and orientation in space. For their implementation, it is necessary to preserve the function of the motor centers of the brain stem not lower than the level of the midbrain. These reflexes are triggered from the receptors of the vestibular apparatus: rectilinear acceleration reflexes arise from the receptors of the otolithic apparatus, and rotation reflexes arise from the receptors of the ampullae of the semicircular canals.
An example of a straight-line acceleration reflex is the elevator reflex. When an elevator begins a rapid ascent (or a downward elevator stops), the tone of the flexor muscles in the lower extremities increases. When the elevator begins to descend (or stops the elevator moving up), the tone of the extensor muscles increases.
Statokinetic rotation reflexes involve the body musculature and the eye muscles. The movement of the eyeballs (ocular nystagmus) helps maintain visual orientation and has two phases.
When the rotation accelerates, first there is a slow deviation of the eyeballs in the direction opposite to the rotation. After this, they quickly bow back (in the direction of rotation). The slow deviation is caused by the receptors of the semicircular canals, the fast component is associated with the influence of the cortical centers.
When the rotation slows down, slow eye movement is directed in the direction of rotation, and fast eye movement is directed against the direction of rotation.
The study of nystagmus is used to assess the functional state of the vestibular apparatus. Ocular nystagmus can occur without rotation if the receptors of the semicircular canals are irritated by a pathological process.
▓ Locomotor function
. In addition to regulating muscle tone, posture and balance, brainstem structures are involved in the control of spinal automaticity of walking and, therefore, in the implementation of locomotion - a set of coordinated movements. The wedge-shaped nucleus of the midbrain is important in performing this function. This nucleus has efferent output to the pontine nuclei. In addition, the functions of the sphenoid nucleus are directly influenced by the cortical regions and the hypothalamus. Destruction of the core leads to loss of the ability to run and walking is severely impaired. When the influence on the nucleus of the overlying parts of the brain is disrupted, voluntary movements disappear. When the connection between the midbrain and the medulla oblongata is disrupted, decerebrate rigidity develops (a sharp predominance of the tone of the extensor muscles over the flexors of the limbs, trunk and neck).
► Coeruleus function
. The locus coeruleus is found only in mammals. It is located in the caudal midbrain and is the main noradrenergic formation of the midbrain. The axons of the neurons of the locus coeruleus are connected with the cerebral cortex, the nuclei of the brainstem, the diencephalon and the motor centers of the spinal cord. The locus coeruleus receives afferent inputs from the nuclei of the trigeminal nerve, the nucleus of the solitary tract, the hypothalamus, the reticular formation of the brainstem, and the substantia nigra of the midbrain.
▓ Motor functions of the locus coeruleus
. The axons of the locus coeruleus neurons go to the ά-motoneurons of the anterior horns of the spinal cord, where norepinephrine inhibits these motor neurons. The impulse activity of locus coeruleus neurons is increased in the REM sleep phase. With unilateral destruction of the locus coeruleus, rotational movements occur in the direction opposite to the destruction, which is explained by the connection of the locus coeruleus with the substantia nigra.
▓ Homeostatic function of the locus coeruleus
. Functionally, the locus coeruleus is associated with the sensory nuclei of the trigeminal, glossopharyngeal and vagus nerves. Together they constitute the basic brain structure that ensures the body's internal environment remains constant (homeostasis). This ability is due to the fact that the locus coeruleus, on the one hand, is able to respond to changes in the gas composition of blood and cerebrospinal fluid, and on the other hand, has numerous efferent outputs to the hypothalamus, reticular formation and autonomic centers, providing neurohumoral regulation of the composition of the internal environment of the body. The locus coeruleus plays a special role in increasing the body's resistance to stress.
► Antinociceptive function of the brainstem
. The brainstem contains structures that are part of the brain's anti-pain system. These include the central gray matter of the midbrain, the large raphe nucleus and part of the giant cell reticular nucleus of the medulla oblongata. Most of the neurons of these formations are serotonergic and have an inhibitory effect on the neurons of the dorsal horns of the spinal cord, which form the pain pathways (lateral spinothalamic and spinoreticular).
► Conductive function of the brain stem
. This function is performed by ascending and descending pathways. Some of these paths are transitive, and some are switched in stem centers.
▓ Ascending (afferent) pathways
are part of the conductive section of analyzers that transmit information from receptors to the sensory zone of the cortex. There are two ascending systems in the brainstem: specific and nonspecific.
▒ Specific afferent system
makes up the lemniscothalamic tract, in which the medial and lateral loops are distinguished.
╠
The medial lemniscus
is formed mainly from the axons of neurons of the Gaulle and Burdach nuclei, which conduct proprioceptive, tactile and visceral sensitivity from the receptors of the limbs, trunk and neck. The medial lemniscus also receives fibers from the spinothalamic tract, which carry tactile sensation; part of the fibers of the nuclei of the V pair of the cranial nerves, conducting proprioceptive and tactile sensitivity from the head; part of the fibers of the nucleus of the solitary tract, conducting taste and visceral sensitivity (fibers of the vagus, glossopharyngeal and facial nerves); part of the fibers of the lateral spinothalamic tract that carry acute localized pain sensation. All fibers of the medial lemniscus switch in specific nuclei of the thalamus.
╠ Lateral
The (auditory)
loop
is composed of axons of neurons in the nuclei of the trapezoid body and the superior olive of the pons, which are part of the conduction section of the auditory analyzer. The lateral loop switches in the medial geniculate body of the thalamus and the inferior colliculi.
The specific conduction system includes the pathways of the visual and vestibular analyzers, which are not included in the lemniscal pathways, but are switched in the sensory nuclei of the thalamus.
A functional feature of a specific conduction system is the high speed of excitation; its neurons have small receptive fields and are predominantly monosensory. In the switching centers of afferent neurons there is a pronounced topographic projection of the periphery. The result is rapid transmission of information with subtle differences in the properties of the stimulus. In this case, evoked potentials, called the primary response, arise in the cortical section of the corresponding analyzer with a short latent period.
▒ Nonspecific ascending pathways
switch in nonspecific nuclei of the thalamus. These are mainly fibers of the lateral spinothalamic and spinoreticular tracts, which conduct temperature and pain sensitivity. A functional feature of a nonspecific system is the slow transmission of information with poor localization of the stimulus and analysis of its properties. The receptive fields of neurons are large, the neurons are polysensory, associated with several types of sensitivity, the topography of the projection of the periphery in the centers is not expressed. When excitation is carried out through this system, evoked potentials with a long latency period, called a secondary response, are recorded on the EEG. The nonspecific system receives collateral fibers from the specific system, which ensures the connection of these two afferent systems.
In addition to conducting excitation through specific and nonspecific afferent systems, the dorsal spinocerebellar tract of Flexig, which carries impulses from receptors of muscles and ligaments, and the ventral spinal cerebellar tract of Govers, from receptors of tendons, skin and internal organs, as well as the vestibulocerebellar tract, pass through the brain stem into the cerebellum. pathway carrying information from vestibular receptors.
▓ Descending pathways of the brain stem can be combined into several groups.
▒ Motor pyramidal tracts
, begin from the Betz cells of the precentral gyrus cortex. They innervate motor neurons of the anterior horns of the spinal cord (corticospinal tract) or motor neurons of the motor nuclei of the cranial nerves (corticobulbar tract), providing voluntary contractions of the muscles of the limbs, trunk, neck and head.
▒ Corticorubral and corticoreticular pathways
at the level of the brain stem they form an extrapyramidal system, the main function of which is the voluntary and reflex regulation of muscle tone, posture and balance. The fibers of these pathways end in the motor centers of the brain stem.
▒ The brainstem contains descending pathways that provide motor functions to the cerebellum. These include the cortico-cerebellar pathway
, through which impulses from the motor cortex enter the cerebellum. This impulse is processed in the cerebellar cortex and its nuclei, and then enters the motor nuclei of the brain stem (red, vestibular, reticular).
The tectospinal tract passes through the brainstem
, which begins in the quadrigeminal region. It provides motor reactions of the body in indicative visual and auditory reflexes.
A diagram of the main motor centers of the brainstem and their pathways is shown below.
Fig.2. Diagram of the main motor centers of the brain stem and their pathways that regulate the tone of the muscles of the trunk and limbs:
KN – red nucleus and rubrospinal tract; ROM – reticular nuclei of the pons and medial reticulospinal tract; VN – vestibular nuclei and vestibulospinal tract; RGN – reticular giant cell nucleus and lateral reticulospinal tract; MN – spinal motor neurons.