General information
The brain contains 25 billion neurons that make up the gray matter. The weight of the organ varies depending on gender. For example, in men its weight is about 1375 g, in women - 1245 g. On average, its share in the total body weight is 2%. At the same time, scientists have found that the level of intellectual development is not related to brain mass. Mental abilities are affected by the number of connections created by the organ. Brain cells are neurons and glia. The former generate and transmit impulses, the latter perform additional functions. There are cavities inside the brain. They are called ventricles. The cranial nerves extend from the organ we are considering to different parts of the human body. They are paired. In total, 12 pairs of nerves depart from the brain. The brain is covered by three membranes: soft, hard and arachnoid. There are spaces between them. They circulate cerebrospinal fluid. It acts as an external hydrostatic environment for the central nervous system and also ensures the removal of metabolic products. The membranes of the brain differ in their structure and the number of vessels passing through them. However, they all provide protection for the contents of the upper part of the skull from mechanical damage.

Pathology of intracranial sinuses
Diseases of these vascular formations are most often caused by their occlusion, which can be caused by thrombosis, thrombophlebitis, or tumor compression of intracranial vessels.
Inflammatory diseases of brain structures can occur when infectious agents enter the venous blood stream (purulent emboli). The infection can be brought to the membranes of the brain from the superficial venous vessels of the skull. In this case, the development of a clinical picture of acute meningitis and encephalitis is possible.
In young children, a picture of neurotoxicosis develops.
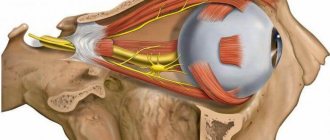
Sometimes neurosurgeons may suspect a fracture of the base of the skull when they see a picture of pulsating exophthalmos. When injured, the internal carotid artery associated with the cavernous canal is damaged. A stream of arterial blood, entering the ophthalmic veins associated with this sinus, causes pulsation, severe redness and protrusion of the eyeball. This pathology is otherwise called carotid-cavernous anastomosis, and this is one of the rarest conditions when listening to the head with a phonendoscope allows you to hear the sounds of blood in the area of the anastomosis.
When the walls of the sinus are damaged, a number of neurological symptoms appear due to damage to nearby branches and nuclei of the cranial nerves. With pathology of the cavernous sinus, oculomotor disorders and the development of trigeminal neuralgia may occur.
If the patient suffers from frequent attacks of headaches or intracranial hypertension, the development of reverse (retrograde) blood flow is possible - from the brain cavity to the superficial veins of the skull. Therefore, in children with intracranial hypertension, the pattern of veins on the scalp is clearly visible.
Due to the flow of blood, the pressure inside the skull decreases. This is a compensatory mechanism for reducing intracranial pressure.
The cerebral sinuses are an important component of the cerebral venous network. Knowing their functions, structural features and localization, experts can assume the development of pathology in a certain area of the brain. To clarify the diagnosis, magnetic resonance imaging with intravascular injection of a contrast agent is necessary.
Spider MO
Arachnoidea encephali is separated from the dura mater by the capillary network of the subdural space. It does not go into the depressions and grooves, like the vascular one. However, the arachnoid membrane spreads over them in the form of bridges. As a result, a subarachnoid space is formed, which is filled with clear fluid. In some areas, mainly at the base of the brain, there is particularly good development of the subarachnoid spaces. They form deep and wide containers - tanks. They contain cerebrospinal fluid.
Vascular (soft) MO
Pia mater encephali directly covers the brain surface. It is presented in the form of a transparent two-layer plate, which extends into the cracks and grooves. The vascular MO contains chromatophores—pigment cells. Especially many of them have been identified at the base of the brain. In addition, there are lymphoid, mast cells, fibroblasts, numerous nerve fibers and their receptors. Parts of soft MO accompany arterial vessels (medium and large), reaching arterioles. Between their walls and the shell there are Virchow-Robin spaces. They are filled with cerebrospinal fluid and communicate with the subarachnoid space. Elastic and collagen fibrils are thrown through them. Vessels are suspended from them, through which conditions are created for their displacement during pulsation without affecting the brain matter.
It is characterized by special strength and density. It contains a large number of elastic and collagen fibers. The hard shell is formed by dense connective tissue.
Tanks
Brain cisterns are small hollow formations located between the arachnoid and pia mater and containing spinal cerebrospinal fluid. All tanks are connected to each other through various holes. These sacs also communicate with the fourth ventricle of the brain.
Anatomy
The anatomical features of the cisterns are that they completely repeat the surface relief of the telencephalon - the gyri and sulci. These formations are narrow and almost flat oblong passages. In some areas they expand and turn into full-fledged containers of cerebrospinal fluid.
Types of tanks
There are the following types of tanks:
- Cerebellar. This tank is the largest among all the others. It is located between the cerebellum and the medulla oblongata. The posterior wall of this cavity is limited by an arachnoid membrane.
- Basal. Represented in the form of a pentagon.
- Prepontinnaya. It lies in front of the bridge. The basilar artery passes through it, giving its branches to the cerebellum.
- Quadrigeminal cistern. It is located between the cerebellum and the corpus callosum.
- Bypass or enveloping cistern of the brain. This tank looks like a canal running along the sides of the cerebellar peduncles. It is subsequently connected to the previous cavity.
Pathologies and diseases
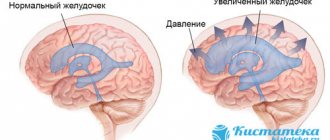
There are very few individual tank diseases. Cavity pathologies occur only in complex syndromes, including hydrocephalus - dropsy of the brain. With this disease, the cisterns, along with the ventricles and other hollow spaces, become pathologically dilated.
When diagnosing, doctors use cerebrospinal fluid and determine the following changes:
- changes in cerebrospinal fluid pressure;
- degree of patency of the subarachnoid space;
- liquid transparency;
- liquor color;
- content of proteins, sugar and other elements.
More information about changes in the cerebrospinal fluid can be found in the article “CSF syndromes.”
Another pathology is a cerebrospinal fluid cyst. This is a disease that is accompanied by the formation of a benign tumor. The following symptoms of a cyst are distinguished:
- Severe headaches, vomiting.
- Loss of coordination in the work of muscles and eyes.
- Mental disorders of an organic nature: illusions, hallucinations of a predominantly auditory and visual nature.
- Partial seizures.
When studying the disease, experts pay special attention to the specifics of the cerebrospinal fluid. You can learn more about how it changes from the article “arachnoid changes of a liquor cystic nature.”
Peculiarities
The hard shell lines the inside of the cranial cavity. At the same time, it acts as its internal periosteum. In the area of the foramen magnum in the occipital part, the dura mater passes into the dura mater of the spinal cord. It also forms the perineural sheath for the cranial nerves. Penetrating into the holes, the shell fuses with their edges. The connection with the bones of the arch is fragile. The shell is easily separated from them. This causes the possibility of epidural hematomas. In the area of the cranial base, the shell fuses with the bones. Particularly strong fusion is observed in the areas where the elements connect to each other and the exit of the cranial nerves from the cavity. The inner surface of the shell is lined with endothelium. This determines its smoothness and pearlescent hue. In some areas there is a splitting of the shell. Here its processes are formed. They protrude deeply into the cracks that separate parts of the brain. Triangular canals are formed in the areas where the processes originate, as well as in the places of attachment to the bones of the internal cranial base. They are also covered with endothelium. These channels are the sinuses of the dura mater.
It is considered the largest process of the shell. The sickle penetrates the longitudinal fissure between the left and right hemispheres, without reaching the corpus callosum. It is a thin sickle-shaped plate in the form of 2 leaves. The superior sagittal sinus lies in the split base of the process. The opposite edge of the sickle has a thickening also with two petals. They contain the inferior sagittal sinus.
Violations of structures
Pathologies of these choroid plexuses arise due to their blockage, which in turn is provoked by thrombosis, thrombophlebitis or compressive neoplasm of intracranial veins and arteries.
Inflammation of the structures of the main human organ can appear when infectious agents penetrate into the bloodstream (all kinds of unconnected vascular substrate, solid, liquid or vapor, circulating through the bloodstream, uncharacteristic in a normal state, capable of provoking blockage of an artery at a fairly large distance from the site of occurrence). The pathological agent can enter the meninges and the vascular beds of the head bone tissue on its surface . In this case, symptoms of peak manifestations of meningitis and other pathologies are likely to appear. In preschool children, a picture of neuropoisoning appears.
In some cases, neurosurgeons can determine damage to the base of the skull by seeing signs of intense exophthalmos. When a fracture occurs, the integrity of the internal carotid artery, which is in contact with the cavernous duct, is disrupted. The flow of venous blood, penetrating into the ophthalmic veins related to this reservoir, provokes pulsation, obvious hyperemia and protrusion of the apple of the optic organ. This deviation is otherwise called the carotid-cavernous anastomosis, and this is one of the extremely rare pathologies when listening to the skull with a phonendoscope makes it possible to hear the noise of blood flow in the area where the vessels join.
Connection with elements of the cerebellum
In the anterior part, the sickle is fused with the cockscomb on the ethmoid bone. The posterior region of the process at the level of the occipital internal protrusion connects with the tentorium of the cerebellum. He, in turn, hangs over the cranial fossa like a gable tent. It contains the cerebellum. Its tentorium penetrates the transverse fissure in the cerebrum. Here it separates the cerebellar hemispheres from the occipital lobes. There are irregularities on the leading edge of the tentorium. Here a notch is formed, to which the brain stem adjoins in front. The lateral portions of the tentorium fuse with the edges of the groove in the posterior sections on the transverse sinus of the occipital bone and with the upper edges of the pyramids on the temporal bones. The connection extends to the posterior processes of the wedge-shaped element in the anterior parts on each side. The cerebellar falx is located in the sagittal plane. Its leading edge is free. It separates the cerebellar hemispheres. The posterior part of the falx is located along the occipital internal crest. It extends to the edge of the large hole and covers it with two legs on both sides. At the base of the falx there is the occipital sinus.
Sinuses of the dura mater
They are sinuses formed as a result of the splitting of the dura mater into two leaves. The sinuses of the brain act as peculiar vessels. Their walls are formed by plates. The sinuses and veins of the brain have a common feature. Their inner surface is lined with endothelium. Meanwhile, the sinuses of the brain and blood vessels differ directly in the structure of the walls. The latter are elastic and include three layers. When cut, the lumen of the veins collapses. The walls of the sinuses, in turn, are stretched tightly. They are formed by fibrous dense connective tissue, which contains elastic fibers. When cut, the lumen of the sinuses gapes. In addition, there are valves in the venous vessels. In the cavity of the sinuses there are several incomplete bars and wavy bars. They are covered with endothelium and spread from wall to wall. In some sinuses these elements are distinguished by significant development. There are no muscle elements in the walls of the sinuses. The sinuses of the dura mater have a structure that allows blood to flow freely under the influence of its gravity, regardless of fluctuations in intracranial pressure.
The following sinuses of the dura mater are distinguished:
- Sinus sagittalis superior. The superior sagittal sinus runs along the superior edge of the greater falx, from the cock's crest to the occipital internal protuberance.
- Sinus sagittalis inferior. The inferior sagittal sinus is located in the thickness of the free edge of the greater falx. It flows into the sinus rectus posteriorly. The connection is located in the area where the lower edge of the greater falx fuses with the anterior edge of the cerebellar tentorium.
- Sinus rectus. The straight sinus is located in the splitting of the tentorium along the line of attachment of the large falx to it.
- Sinus transversus. The transverse sinus is located at the origin of the tentorium cerebellum from the membrane of the brain.
- Sinus occipitalis. The occipital sinus lies at the base of the cerebellar falx.
- Sinus sigmoideus. The sigmoid sinus is located in the groove of the same name on the inner cranial surface. It looks shaped like the letter S. In the area of the jugular foramen, the sinus becomes the internal vein.
- Sinus cavernosus. The paired cavernous sinus is located on both sides of the sella turcica.
- Sinus sphenoparietalis. The sphenoparietal sinus is adjacent to the posterior free area on the lesser wing of the sphenoid bone.
- Sinus petrosus superior. The superior petrosal sinus is located at the superior edge of the temporal bone.
- Sinus petrosus inferior. The inferior petrosal sinus is located between the clivus of the occipital and the pyramid of the temporal bones.
Cavernous sinus thrombosis: types and causes
Cavernous sinus thrombosis (ICD-10 code - G08) can occur due to various reasons, especially because it can be a complication of almost any disease state.
!
Having studied the pathogenesis of the disease, medicine, first of all, distinguishes its two types: non-infectious and infectious.
In turn, all possible causes of thrombosis belong to one or another type.
First of all, we will consider aseptic thrombosis of the cavernous sinus. At this point in time, it is considered more common than septic. The following reasons predispose to its development:
- any traumatic brain injuries of the head (damage to the tissues of the head and skull, as well as intracranial injuries);
- complications of any surgical and direct neurosurgical interventions;
- brain tumors;
- obstruction of the internal jugular vein;
- complications of spinal or epidural anesthesia;
- hormonal dysfunction and therapy, taking oral contraceptives;
- heart failure, heart rhythm disturbances, heart defects;
- nephrotic syndrome;
- dehydration of the body;
- diseases of the coagulation system;
- thrombophilia;
- cirrhosis of the liver;
- frequent abortions;
- vasculitis, etc.
Septic thrombosis of the cavernous sinus can also be of completely different origins - both bacterial, viral and rhinogenic etiology. Below we give reasons that may be provoking factors for the development of the disease:
- intracranial abscesses;
- bacterial infection;
- viral infection;
- fungal infection;
- diseases caused by parasites.
Infectious thrombosis of the cavernous sinus is often otogenic in nature. This means that the disease began after infection of the middle ear cavities.
Video and cavernous sinus thrombosis. Source - Natalya Lozi
Sinus sagittalis superior
In the anterior sections, the superior sinus anastomoses (connects) with the veins of the nasal cavity. The posterior part flows into the transverse sinus. To the left and right of it there are lateral lacunae communicating with it. They are small cavities located between the outer and inner layers of the dura mater. Their number and size are very different. The lacunae communicate with the cavity of the sinus sagittalis superior. They include vessels of the dura mater and brain, as well as diploic veins.
MRI of cerebral vessels: arteriography, venography
Magnetic resonance imaging is a method of layer-by-layer scanning of the study area through a given number of millimeters. Comparison and analysis of hundreds of tomograms obtained is carried out by software.
The predominant analysis of blood vessels using magnetic resonance scanning is MR angiography (MRA).
How does MRI of the brain differ from MRI of blood vessels? The first examination is carried out to carefully examine the cerebral parenchyma, sella turcica, nerve fibers, and pituitary gland. It is prescribed to identify tumors, cysts, dilation of venous sinuses, inflammatory foci, edema, hemorrhage, and hematomas. The second type is used primarily to analyze the condition of veins and arteries. The study determines the patency of blood vessels, identifies blood clots, anomalies, malformations, aneurysms, vasculitis, angiomas, and other pathological changes.
The optimal equipment in terms of price and quality, which allows both procedures to be carried out efficiently, is MRI scanners with a power of more than 1.5 Tesla.
Sinus transversus
This sinus is the largest and widest. On the inside of the scales of the occipital bone, it corresponds to a wide groove. Next, the sinus transversus becomes the sigmoid sinus. Then it goes into the mouth of the internal jugular vessel. Sinus transversus and Sinus sigmoideus thus act as the main venous collectors. At the same time, all other sinuses flow into the first. Some venous sinuses enter it directly, some indirectly. On the right and left, the transverse sinus continues into the sinus sigmoideus of the corresponding side. The area where the venous sinuses sagittalis, rectus and occipitalis flow into it is called the drain.
Sinus cavernosus
Its other name is cavernous sinus. It received this name due to the presence of numerous partitions. They give the sinus the appropriate structure. The abducens, ophthalmic, trochlear, oculomotor nerves, as well as the carotid artery (internal) along with the sympathetic plexus pass through the cavernous sinus. There is a communication between the right and left side of the sinus. It is presented in the form of the posterior and anterior intercavernous sinus. As a result, a vascular ring is formed in the area of the sella turcica. The sinus sphenoparietalis flows into the cavernous sinus (in its anterior sections).
Related Images
The close relationship between the cavernous sinus and the internal carotid artery plays a role in the development and course of some types of pathology of the internal carotid artery, such as carotid-cavernous aneurysms and carotid-cavernous anastomosis.
Tumors of nearby structures (primarily some tumors of the pituitary gland) can lead to compression of the cavernous sinus, which, in turn, will manifest itself as signs of dysfunction of the nerves that pass through it. In particular, such patients experience ophthalmoplegia (disorders of eyeball movement) and sensitivity disorders in the innervation zones of the ophthalmic and maxillary nerve.
Numerous connections of the cavernous sinus with extracranial venous structures can serve as a route for the spread of infection from the soft tissues of the face into the cranial cavity (with the development of sinus thrombosis). Most often, this route is an anastomosis between the facial vein and the veins of the orbit in the medial corner of the eye (the spread of infection is also facilitated by the fact that the facial vein is devoid of valves).
Additionally
In some areas, the sinuses of the membrane form anastomoses with the external venous vessels of the head with the help of graduates - emissary veins. In addition, the sinuses communicate with the diploic branches. These veins are located in the spongy substance in the bones of the cranial vault and flow into the superficial vessels of the head. Blood thus flows through the vascular branches into the dura sinuses. It then drains into the left and right jugular (internal) veins. Due to the anastomoses of the sinuses with diploic vessels, graduates and plexuses, blood can flow into the superficial networks of the face.